

The impact of health information technology on prescribing errors in hospitals: a systematic review and behaviour change technique analysis
- PMID: 33272315
- PMCID: PMC7716445
- DOI: 10.1186/s13643-020-01510-7
The impact of health information technology on prescribing errors in hospitals: a systematic review and behaviour change technique analysis
Abstract
Background: Health information technology (HIT) is known to reduce prescribing errors but may also cause new types of technology-generated errors (TGE) related to data entry, duplicate prescribing, and prescriber alert fatigue. It is unclear which component behaviour change techniques (BCTs) contribute to the effectiveness of prescribing HIT implementations and optimisation. This study aimed to (i) quantitatively assess the HIT that reduces prescribing errors in hospitals and (ii) identify the BCTs associated with effective interventions.
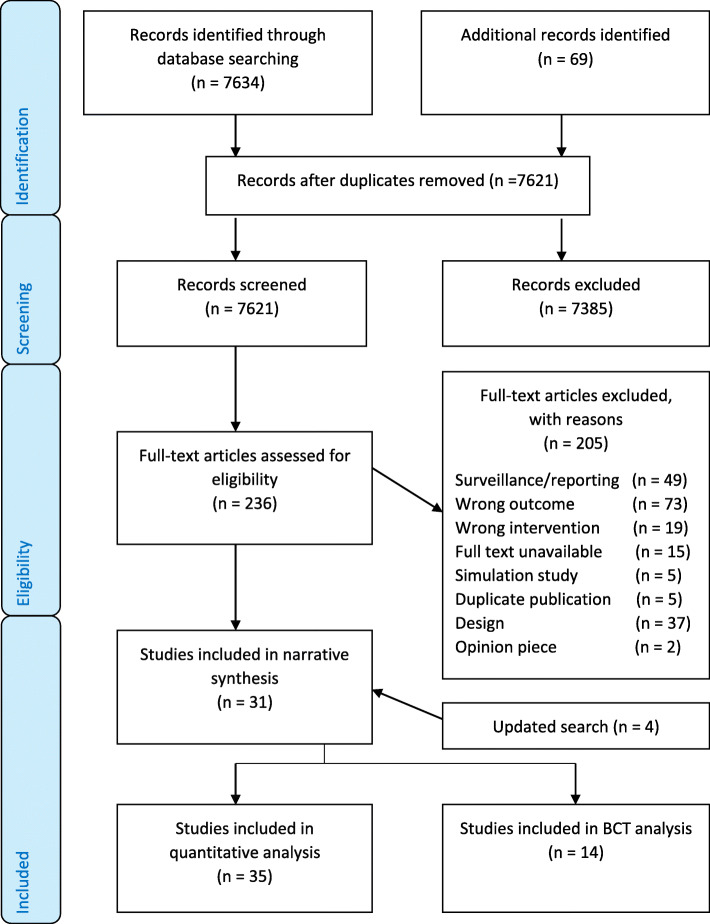
Methods: Articles were identified using CINAHL, EMBASE, MEDLINE, and Web of Science to May 2020. Eligible studies compared prescribing HIT with paper-order entry and examined prescribing error rates. Studies were excluded if prescribing error rates could not be extracted, if HIT use was non-compulsory or designed for one class of medication. The Newcastle-Ottawa scale was used to assess study quality. The review was reported in accordance with the PRISMA and SWiM guidelines. Odds ratios (OR) with 95% confidence intervals (CI) were calculated across the studies. Descriptive statistics were used to summarise effect estimates. Two researchers examined studies for BCTs using a validated taxonomy. Effectiveness ratios (ER) were used to determine the potential impact of individual BCTs.
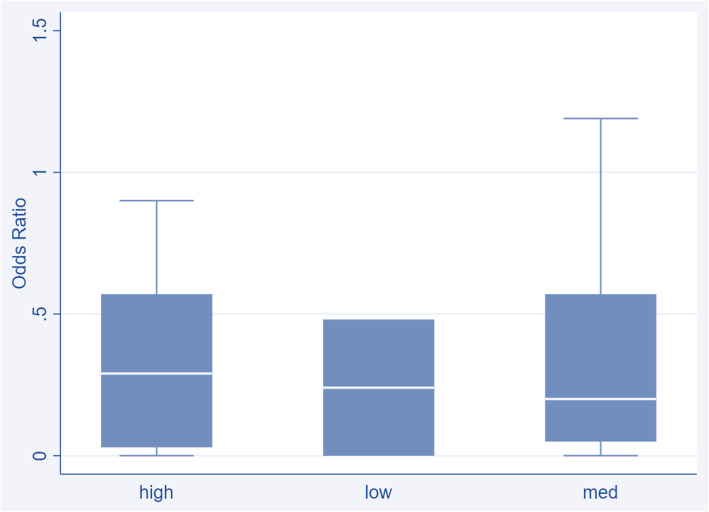
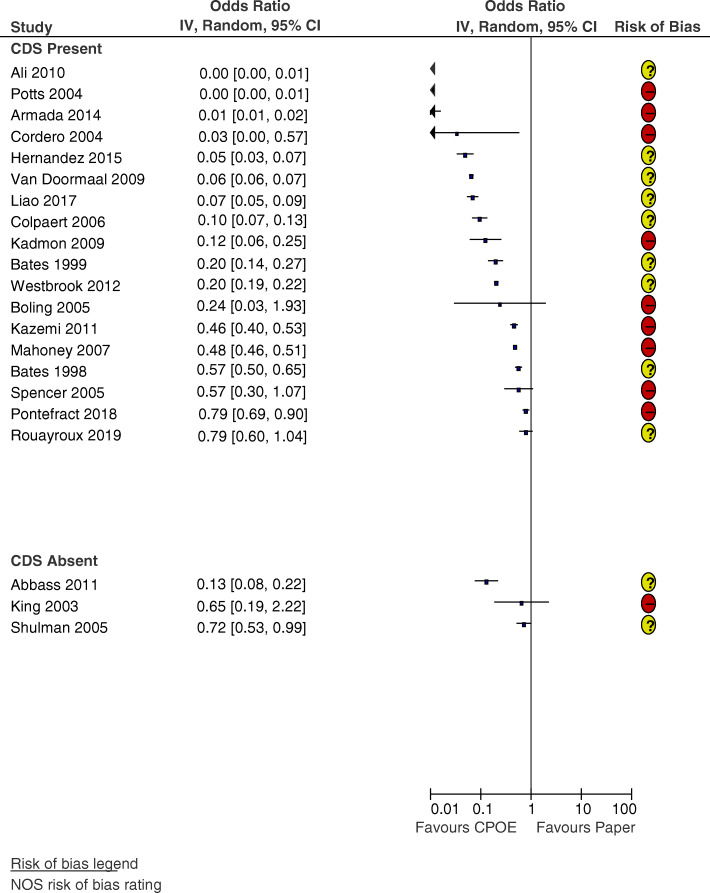
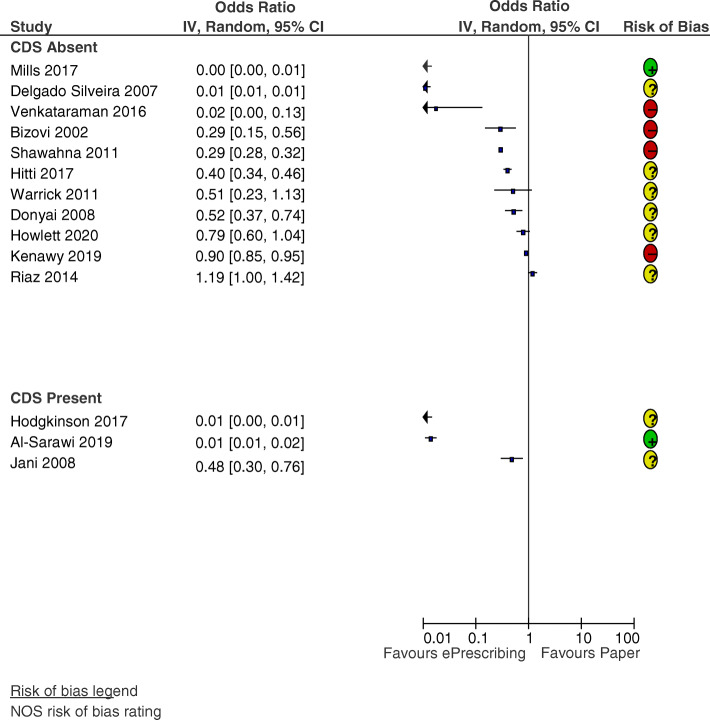
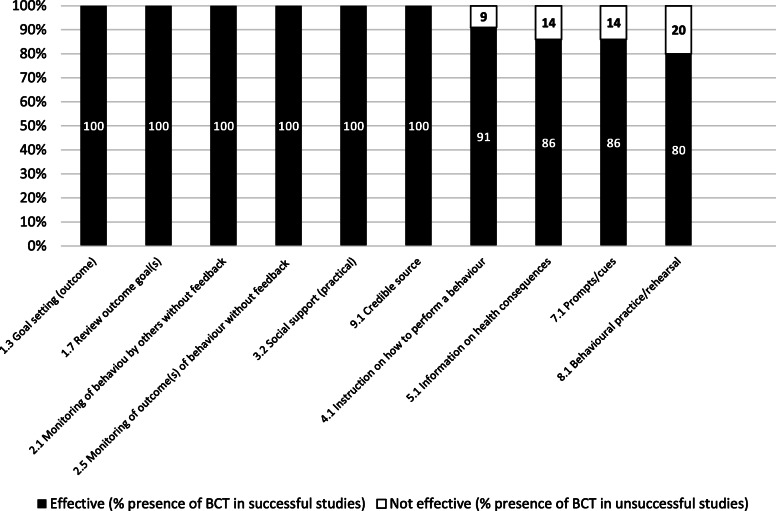
Results: Thirty-five studies of variable risk of bias and limited intervention reporting were included. TGE were identified in 31 studies. Compared with paper-order entry, prescribing HIT of varying sophistication was associated with decreased rates of prescribing errors (median OR 0.24, IQR 0.03-0.57). Ten BCTs were present in at least two successful interventions and may be effective components of prescribing HIT implementation and optimisation including prescriber involvement in system design, clinical colleagues as trainers, modification of HIT in response to feedback, direct observation of prescriber workflow, monitoring of electronic orders to detect errors, and system alerts that prompt the prescriber.
Conclusions: Prescribing HIT is associated with a reduction in prescribing errors in a variety of hospital settings. Poor reporting of intervention delivery and content limited the BCT analysis. More detailed reporting may have identified additional effective intervention components. Effective BCTs may be considered in the design and development of prescribing HIT and in the reporting and evaluation of future studies in this area.
Keywords: BCTTv1; Behaviour change techniques; CPOE; HIT; Prescribing errors; Synthesis without meta-analysis; Technology-generated errors; ePrescribing.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Aitken M, Gorokhovich L. Advancing the responsible use of medicines: applying levers for change. 2012.
-
- Department of Health and Children . eHealth strategy for Ireland. 2013.
-
- Institute of Medicine . In: Preventing medication errors. Philip A, Julie W, Bootman JL, Linda RC, editors. Washington: The National Academies Press; 2007.
-
- Cresswell K, Lee L, Mozaffar H, Williams R, Sheikh A, Team obotNeP Sustained user engagement in health information technology: the long road from implementation to system optimization of computerized physician order entry and clinical decision support systems for prescribing in hospitals in England. Health Serv Res. 2017;52(5):1928–1957. doi: 10.1111/1475-6773.12581. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
