

Racial/Ethnic Disparities in All-Cause Mortality among Patients Diagnosed with Triple-Negative Breast Cancer
- PMID: 33272926
- PMCID: PMC10571320
- DOI: 10.1158/0008-5472.CAN-20-3094
Racial/Ethnic Disparities in All-Cause Mortality among Patients Diagnosed with Triple-Negative Breast Cancer
Abstract
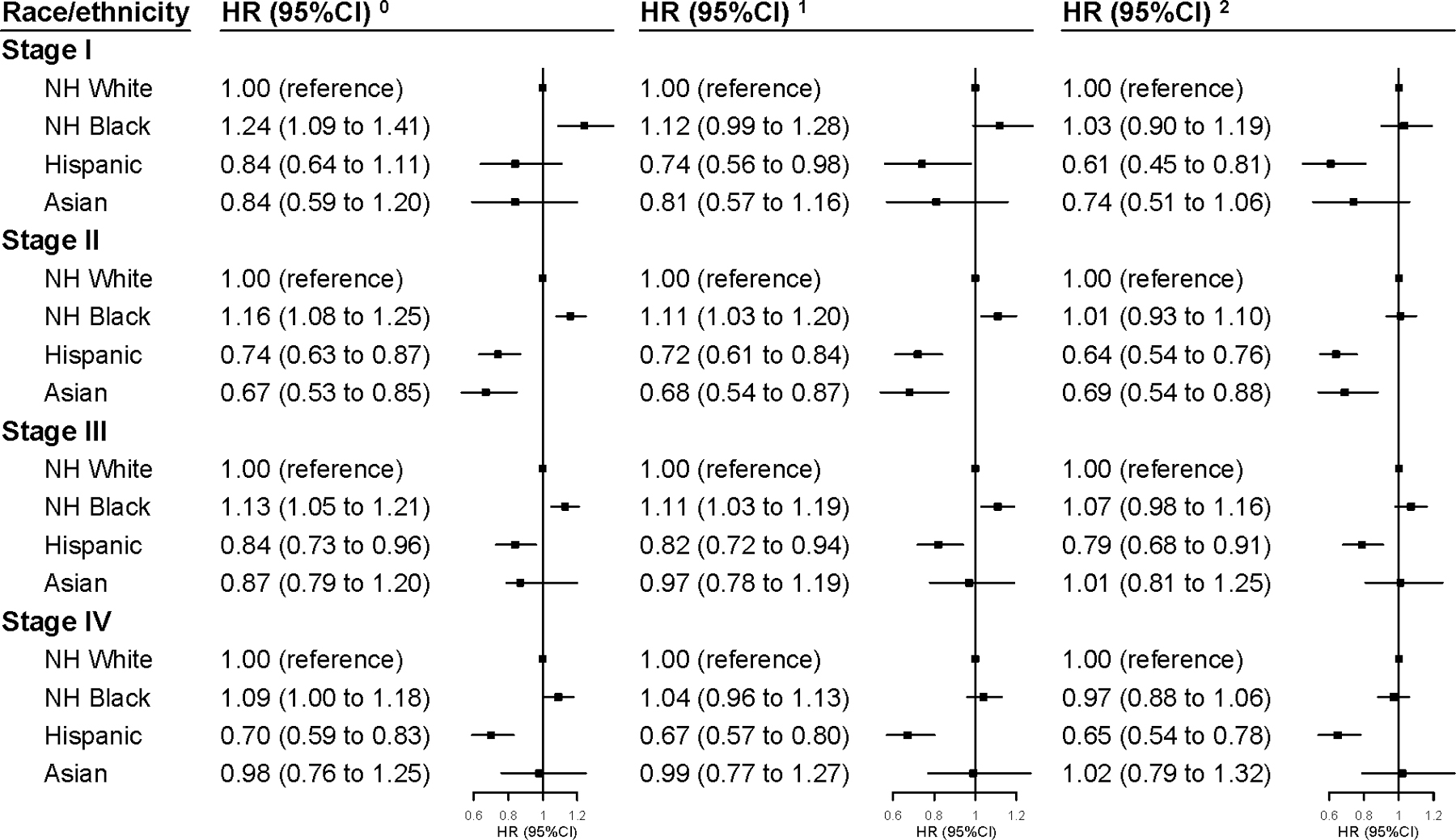
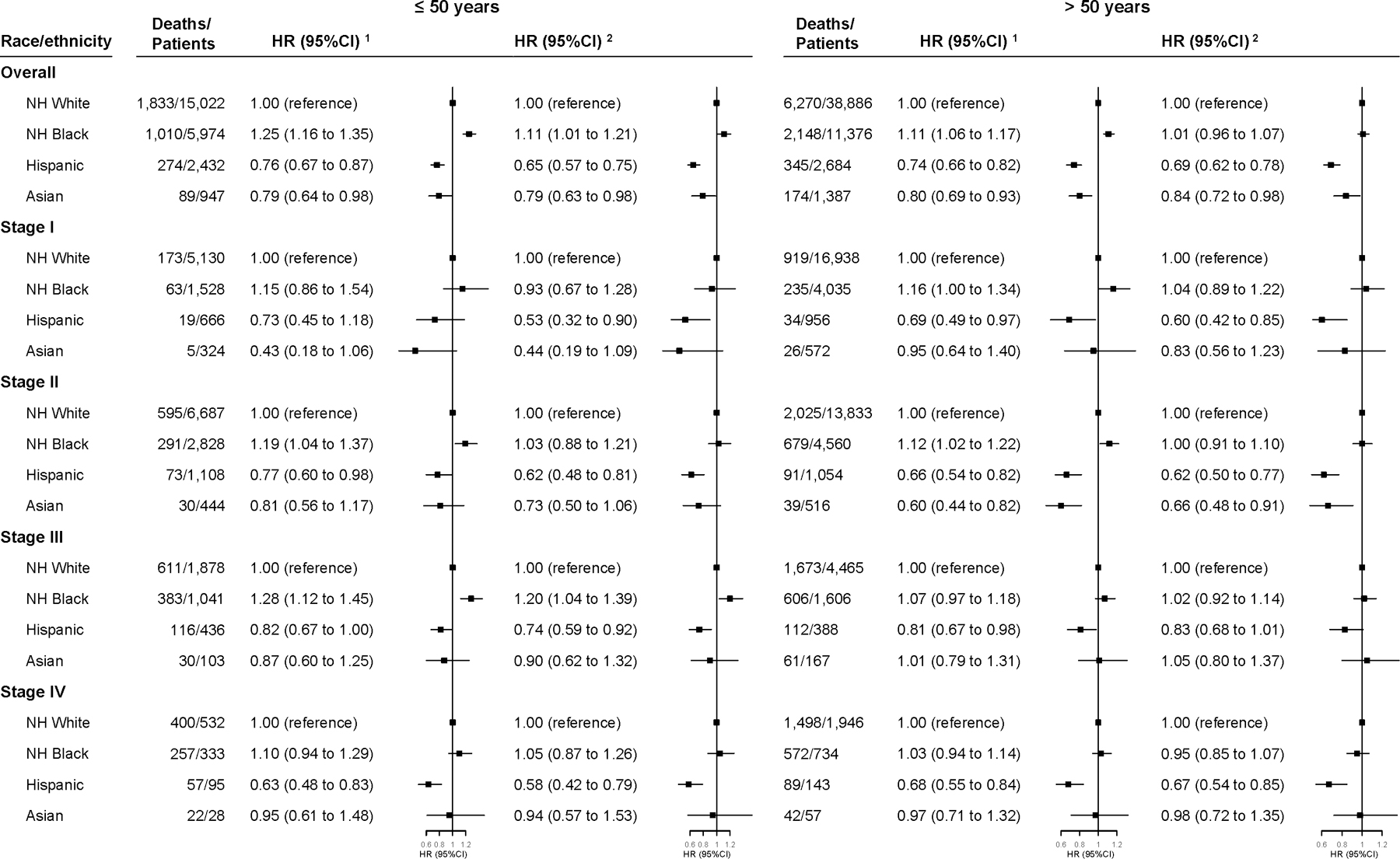
It is unclear whether racial/ethnic disparities in triple-negative breast cancer (TNBC) mortality remain after accounting for clinical characteristics, treatment, and access-to-care-related factors. In this study, women with a primary diagnosis of TNBC during 2010-2014 were identified from the National Cancer Database. Hazard ratios (HR) and 95% confidence intervals (CI) for 3- and 5-year all-cause mortality associated with race/ethnicity were estimated using Cox proportional hazards models with stepwise adjustments for age, clinical characteristics, treatment, and access-to-care-related factors. Of 78,708 patients, non-Hispanic (NH) black women had the lowest 3-year overall survival rates (79.4%), followed by NH-whites (83.1%), Hispanics (86.0%), and Asians (87.1%). After adjustment for clinical characteristics, NH-blacks had a 12% higher risk of dying 3 years post-diagnosis (HR, 1.12; 95% CI, 1.07-1.17), whereas Hispanics and Asians had a 24% (HR, 0.76; 95% CI, 0.70-0.83) and 17% (HR, 0.83; 95% CI, 0.73-0.94) lower risk than their NH-white counterparts. The black-white disparity became non-significant after combined adjustment for treatment and access-to-care-related factors (HR, 1.04; 95% CI, 0.99-1.09), whereas the white-Hispanic and white-Asian differences remained. Stratified analyses revealed that among women aged less than or equal to 50 with stage III cancer, the elevated risk among NH-blacks persisted (HR, 1.20; 95% CI, 1.04-1.39) after full adjustments. Similar results were seen for 5-year mortality. Overall, clinical characteristics, treatment, and access-to-care-related factors accounted for most of the white-black differences in all-cause mortality of TNBC but explained little about Hispanic- and Asian-white differences. SIGNIFICANCE: These findings highlight the need for equal healthcare to mitigate the black-white disparity and for investigations of contributors beyond healthcare for lower mortality among Asians and Hispanics.
©2020 American Association for Cancer Research.
Conflict of interest statement
Figures
References
-
- Foulkes WD, Smith IE, Reis-Filho JS. Triple-negative breast cancer. N Engl J Med 2010;363:1938–48. - PubMed
-
- Cheang MCU, Voduc D, Bajdik C, Leung S, McKinney S, Chia SK, et al. Basal-Like Breast Cancer Defined by Five Biomarkers Has Superior Prognostic Value than Triple-Negative Phenotype. Clin Cancer Res 2008;14:1368–76. - PubMed
-
- Newman LA, Kaljee LM. Health Disparities and Triple-Negative Breast Cancer in African American Women: A Review. JAMA Surg 2017;152:485–93. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
