

Overlapping central and peripheral nervous system syndromes in MOG antibody-associated disorders
- PMID: 33272955
- PMCID: PMC7803332
- DOI: 10.1212/NXI.0000000000000924
Overlapping central and peripheral nervous system syndromes in MOG antibody-associated disorders
Abstract
Objective: Antibodies to myelin oligodendrocyte glycoprotein (MOG) are associated with CNS demyelination inclusive of optic neuritis (ON) and transverse myelitis (TM). To examine whether peripheral nervous system (PNS) involvement is associated with MOG antibody-associated disorders (MOGAD), we performed detailed characterization of an Australasian MOGAD cohort.
Methods: Using a live cell-based assay, we diagnosed 271 adults with MOGAD (2013-2018) and performed detailed clinical and immunologic characterization on those with likely PNS involvement.
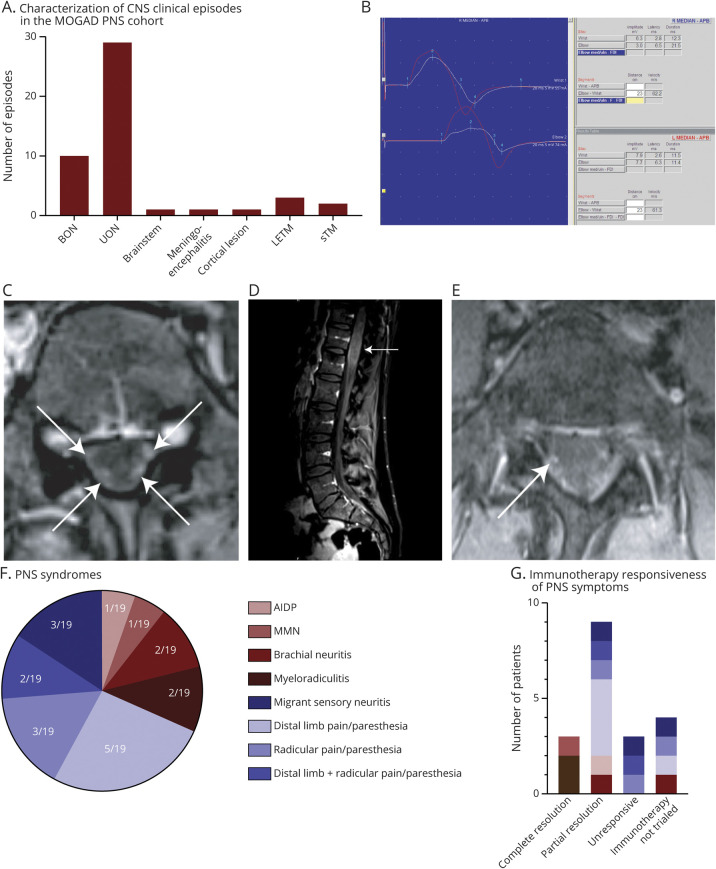
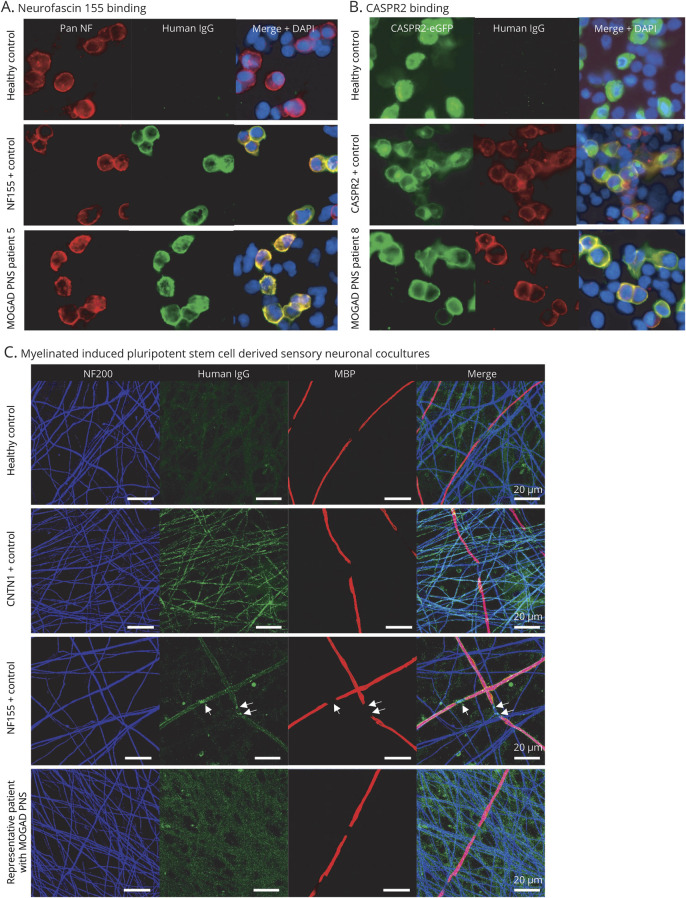
Results: We identified 19 adults with MOGAD and PNS involvement without prior TM. All patients had CNS involvement including ON (bilateral [n = 3], unilateral [n = 3], and recurrent [n = 7]), a cortical lesion (n = 1), meningoencephalitis (n = 1), and subsequent TM (n = 4). Clinical phenotyping and neurophysiology were consistent with acute inflammatory demyelinating polyneuropathy (n = 1), myeloradiculitis (n = 3), multifocal motor neuropathy (n = 1), brachial neuritis (n = 2), migrant sensory neuritis (n = 3), and paresthesia and/or radicular limb pain (n = 10). Onset MRI spine was consistent with myeloradiculitis with nerve root enhancement in 3/19 and normal in 16/19. Immunotherapy resulted in partial/complete PNS symptom resolution in 12/15 (80%) (steroids and/or IV immunoglobulin n = 9, rituximab n = 2, and plasmapheresis n = 1). We identified serum antibodies targeting neurofascin 155, contactin-associated protein 2, or GM1 in 4/16 patients with MOGAD PNS compared with 0/30 controls (p = 0.01). There was no binding to novel cell surface antigens using an in vitro myelinating sensory neuronal coculture model.
Conclusions: Myeloradiculitis, combined central and peripheral demyelination syndromes, and inflammatory neuropathies may be associated with MOGAD and may be immunotherapy responsive. We identified a subgroup who may have pathology mediated by coexistent autoantibodies.
Copyright © 2020 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American Academy of Neurology.
Figures
References
-
- Schluesener HJ, Sobel RA, Linington C, Weiner HL. A monoclonal antibody against a myelin oligodendrocyte glycoprotein induces relapses and demyelination in central nervous system autoimmune disease. J Immunol 1987;139:4016–4021. - PubMed
-
- Brunner C, Lassmann H, Waehneldt TV, Matthieu JM, Linington C. Differential ultrastructural localization of myelin basic protein, myelin/oligodendroglial glycoprotein, and 2',3'-cyclic nucleotide 3'-phosphodiesterase in the CNS of adult rats. J Neurochem 1989;52:296–304. - PubMed
-
- Ramanathan S, Dale RC, Brilot F. Anti-MOG antibody: the history, clinical phenotype, and pathogenicity of a serum biomarker for demyelination. Autoimmun Rev 2016;15:307–324. - PubMed
-
- Reindl M, Waters P. Myelin oligodendrocyte glycoprotein antibodies in neurological disease. Nat Rev Neurol 2019;15:89–102. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous