

Upadacitinib for psoriatic arthritis refractory to biologics: SELECT-PsA 2
- PMID: 33272960
- PMCID: PMC7892371
- DOI: 10.1136/annrheumdis-2020-218870
Upadacitinib for psoriatic arthritis refractory to biologics: SELECT-PsA 2
Abstract
Background: Upadacitinib is a Janus kinase inhibitor under evaluation for the treatment of psoriatic arthritis (PsA). We evaluated upadacitinib in patients with PsA and prior inadequate response or intolerance to at least one biologic disease-modifying antirheumatic drug (DMARD).
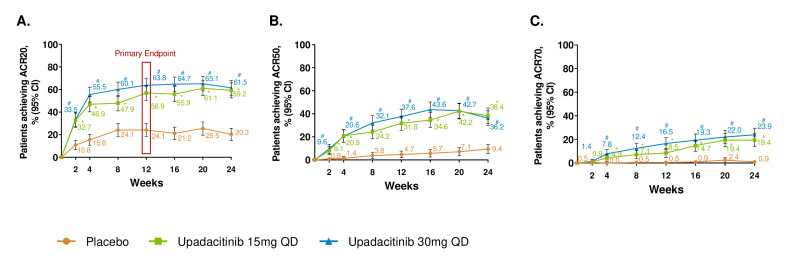
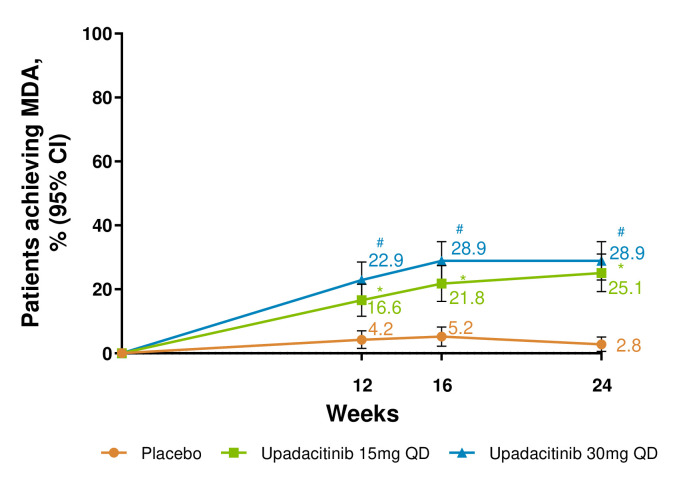
Methods: In this 24-week randomised, placebo-controlled, double-blind, phase 3 trial, 642 patients were randomised (2:2:1:1) to once per day upadacitinib 15 mg or 30 mg, placebo followed by upadacitinib 15 mg or placebo followed by upadacitinib 30 mg at week 24. The primary endpoint was the proportion of patients achieving American College of Rheumatology (ACR) 20 response at week 12. Achievement of minimal disease activity (MDA) was assessed at week 24. Treatment-emergent adverse events are reported for all patients who received at least one dose of trial drug.
Results: At week 12, significantly more patients receiving upadacitinib 15 mg and 30 mg versus placebo achieved ACR20 (56.9% and 63.8% vs 24.1%; p<0.001 for both comparisons). At week 24, MDA was achieved by more upadacitinib 15 mg-treated (25.1%) and 30 mg-treated patients (28.9%) versus placebo (2.8%; p<0.001 for both comparisons). Generally, the rates of treatment-emergent adverse events were similar with placebo and upadacitinib 15 mg and higher with upadacitinib 30 mg at week 24. Rates of serious infections were 0.5%, 0.5% and 2.8% with placebo, upadacitinib 15 mg and upadacitinib 30 mg, respectively.
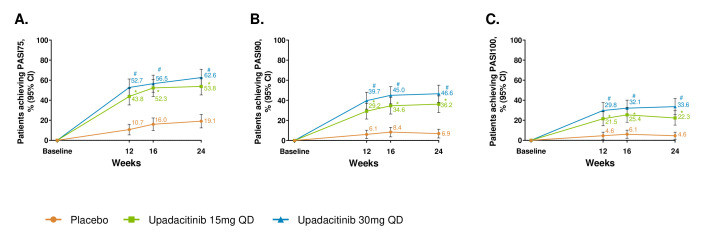
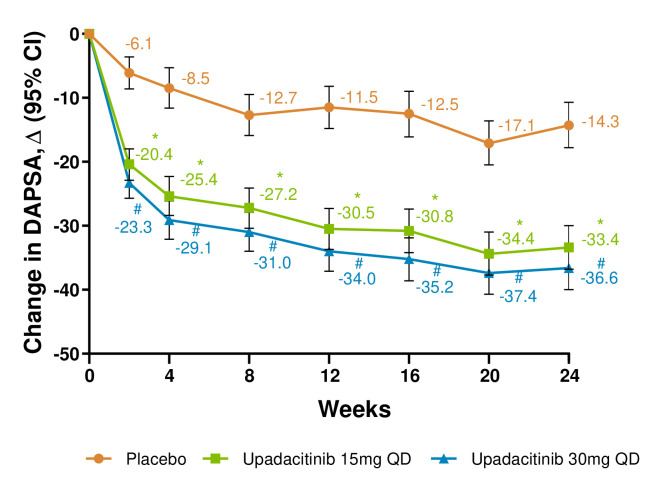
Conclusion: In this trial of patients with active PsA who had inadequate response or intolerance to at least one biologic DMARD, upadacitinib 15 mg and 30 mg was more effective than placebo over 24 weeks in improving signs and symptoms of PsA.
Clinical trial registration number: NCT03104374.
Keywords: arthritis; biological therapy; psoriatic.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: PJM has received research grants, consulting fees and/or speaker’s fees from AbbVie, Amgen, Boehringer Ingelheim, Bristol Myers, Celgene, Eli Lilly, Galapagos, Genentech, Gilead, Janssen, Merck, Novartis, Pfizer, Sun Pharma and UCB. KP received honoraria or fees for advisory board, speaker and consultant services from AbbVie, Amgen, Astellas, Baxalta, Baxter, Boehringer Ingelheim, Bristol Myers Squibb, Celgene, Centocor, Dermira, Eli Lilly, Forward Pharma, Galderma, Genentech, GlaxoSmithKline, Janssen, Kyowa-Hakko Kirin, Leo Pharma, MedImmune, Merck-Serono, Merck Sharp & Dohme, Novartis, Pfizer, Regeneron, Roche, Sanofi-Genzyme, Stiefel, Sun Pharma, Takeda, UCB and Valeant and received research grants from AbbVie, Amgen, Astellas, Baxalta, Boehringer Ingelheim, Bristol Myers Squibb, Celgene, Centocor, Dermira, Eli Lilly, Galderma, Genentech, GlaxoSmithKline, Janssen, Kyowa-Hakko Kirin, Leo Pharma, MedImmune, Merck-Serono, Merck Sharp & Dohme, Novartis, Pfizer, Regeneron, Roche, Sanofi-Genzyme, Stiefel, Takeda, UCB and Valeant. WT received grant/research support from AbbVie, Celgene and Eli Lilly and is a consultant for AbbVie, Celgene, Eli Lilly, Janssen, Novartis, and Pfizer, Speakers bureau: AbbVie, Amgen, Celgene, Eli Lilly, Janssen, Novartis, UCB and Pfizer. FEVdB received speaker and/or consultancy fees from AbbVie, Celgene, Eli Lilly, Janssen, Merck, Novartis, Pfizer and UCB. ST received speaker fees from AbbVie, Asahi Kasei, Chugai, Daiichi Sankyo, Eli Lilly, Eisai, Mitsubishi Tanabe, Celgene and Novartis Pharma. ED received grant/research support from AbbVie, Eli Lilly, Glaxo Smith & Kline, Novartis, Pfizer, UCB Biopharma SPRL, Sanofi – Aventis, Hexal AG, Gilead, R-Pharm, Janssen-Cilag, Galapagos NV. MK has participated in Advisory Boards and/or lectures for Pfizer, Abbott, Actelion, AstraZeneca, Amgen, Roche, Bristol Myers Squibb and Janssen and has received clinical trial honoraria from Pfizer, Amgen, AstraZeneca, Anthera Pharmaceuticals, Bristol Myers Squibb, Biogen Idec, Celltrion, Eli Lilly, Human Genome Sciences, Novartis, Roche, Sanofi, UCB Inc. AL, JKA, XW, SZ, PZ, ALP and RMM are AbbVie employees and may own AbbVie stock or options.
Figures
References
-
- Mease PJ, van der Heijde D, Ritchlin CT, et al. . Ixekizumab, an interleukin-17A specific monoclonal antibody, for the treatment of biologic-naive patients with active psoriatic arthritis: results from the 24-week randomised, double-blind, placebo-controlled and active (adalimumab)-controlled period of the phase III trial SPIRIT-P1. Ann Rheum Dis 2017;76:79–87. 10.1136/annrheumdis-2016-209709 - DOI - PMC - PubMed
-
- Mease P, van der Heijde D, Landewé R, et al. . Secukinumab improves active psoriatic arthritis symptoms and inhibits radiographic progression: primary results from the randomised, double-blind, phase III future 5 study. Ann Rheum Dis 2018;77:890–7. 10.1136/annrheumdis-2017-212687 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
