

Association of Mandatory Bundled Payments for Joint Replacement With Postacute Care Outcomes Among Medicare and Medicaid Dual Eligible Patients
- PMID: 33273296
- PMCID: PMC7855778
- DOI: 10.1097/MLR.0000000000001473
Association of Mandatory Bundled Payments for Joint Replacement With Postacute Care Outcomes Among Medicare and Medicaid Dual Eligible Patients
Abstract
Importance: The Medicare comprehensive care for joint replacement (CJR) model, a mandatory bundled payment program started in April 2016 for hospitals in randomly selected metropolitan statistical areas (MSAs), may help reduce postacute care (PAC) use and episode costs, but its impact on disparities between Medicaid and non-Medicaid beneficiaries is unknown.
Objective: To determine effects of the CJR program on differences (or disparities) in PAC use and outcomes by Medicare-Medicaid dual eligibility status.
Design, setting, and participants: Observational cohort study of 2013-2017, based on difference-in-differences (DID) analyses on Medicare data for 1,239,452 Medicare-only patients, 57,452 dual eligibles with full Medicaid benefits, and 50,189 dual eligibles with partial Medicaid benefits who underwent hip or knee surgery in hospitals of 75 CJR MSAs and 121 control MSAs.
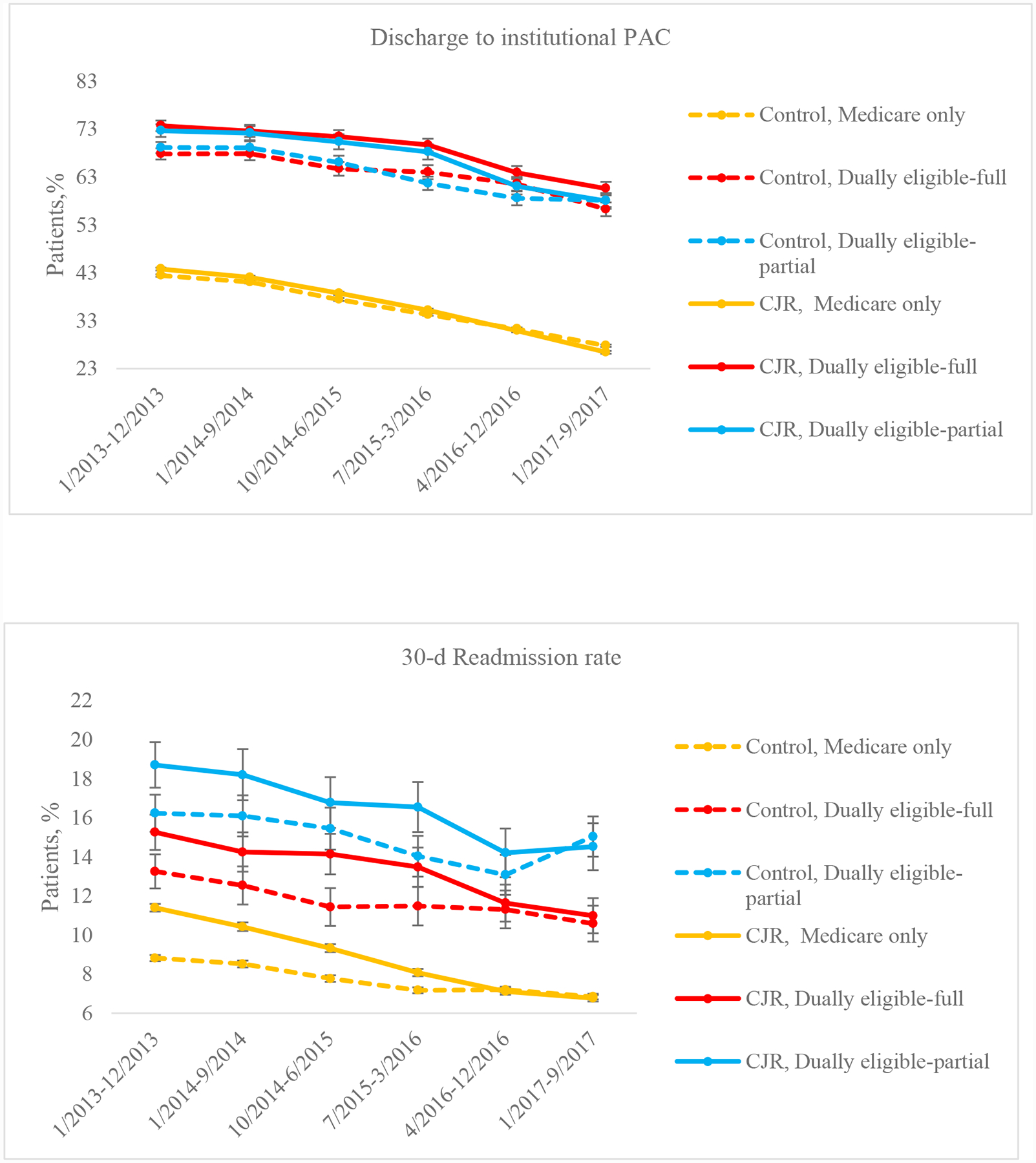
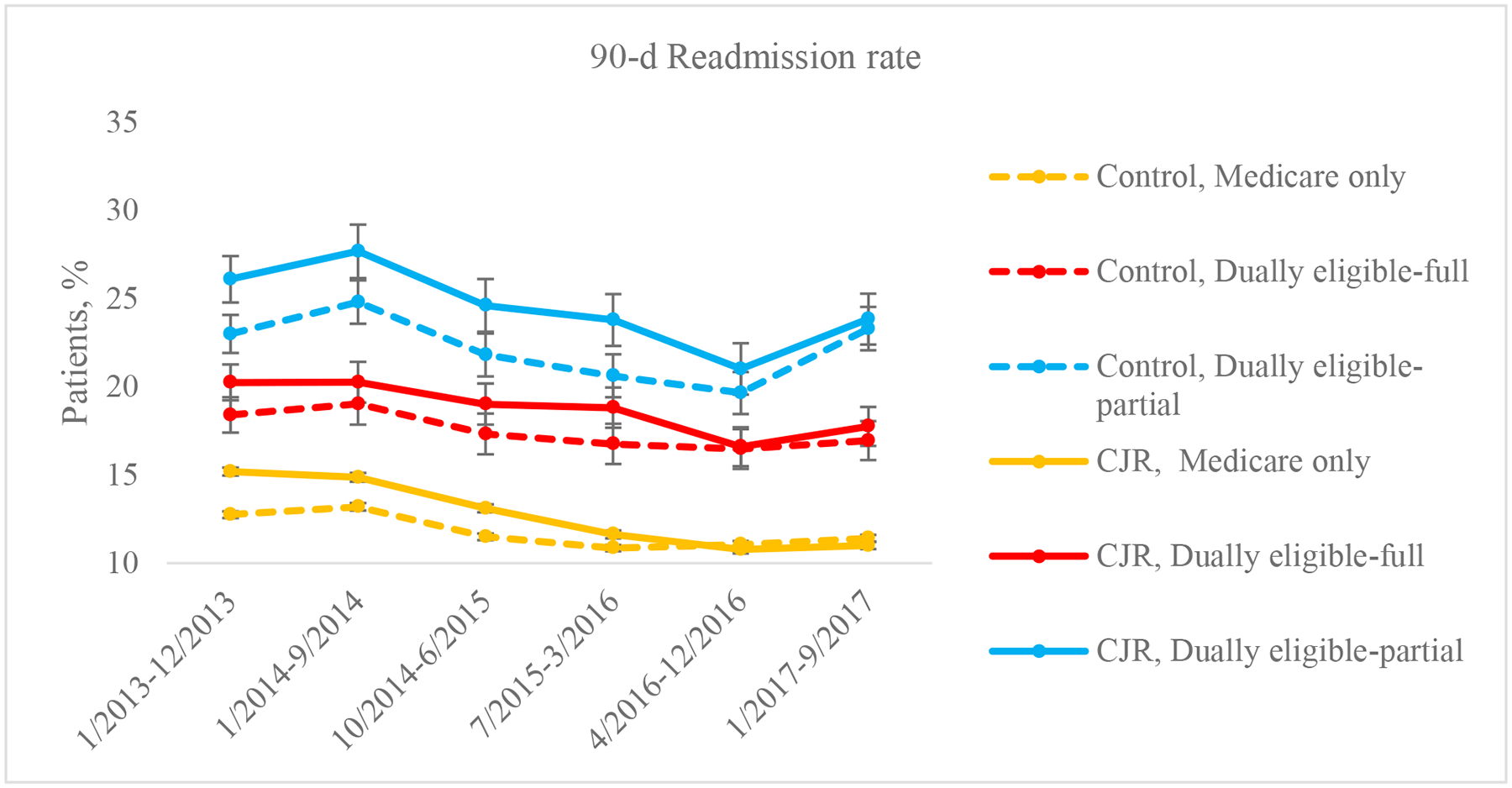
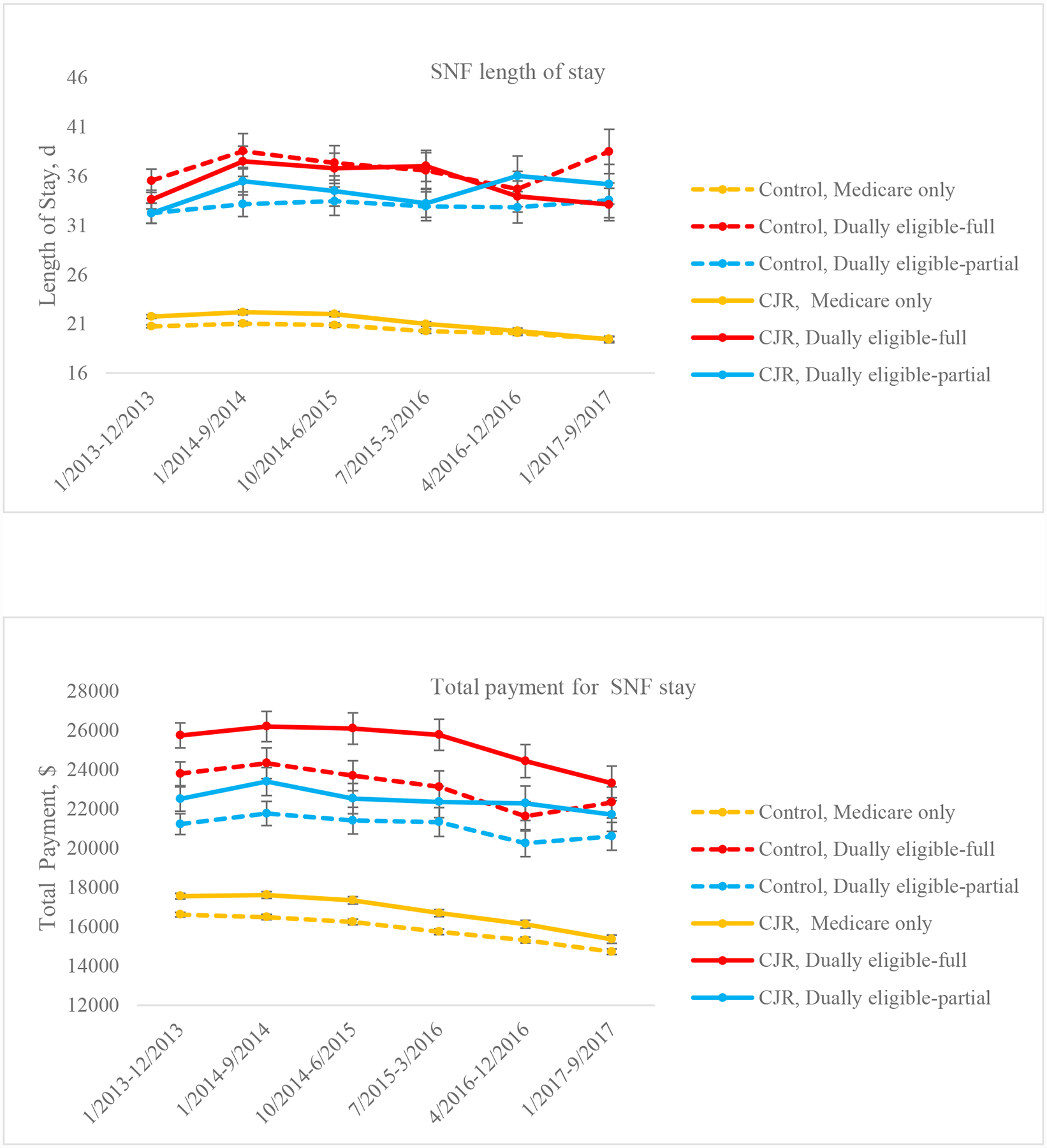
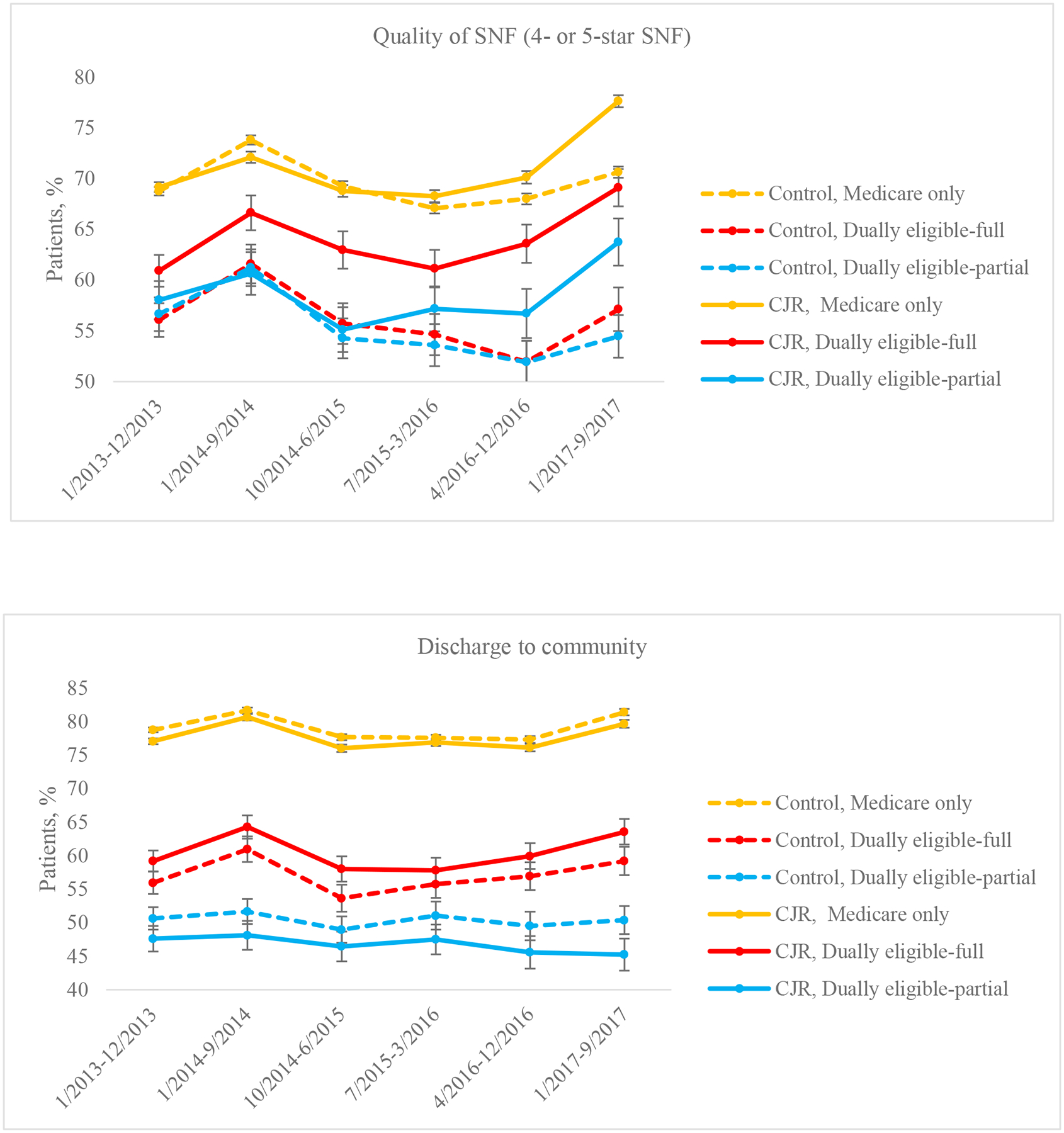
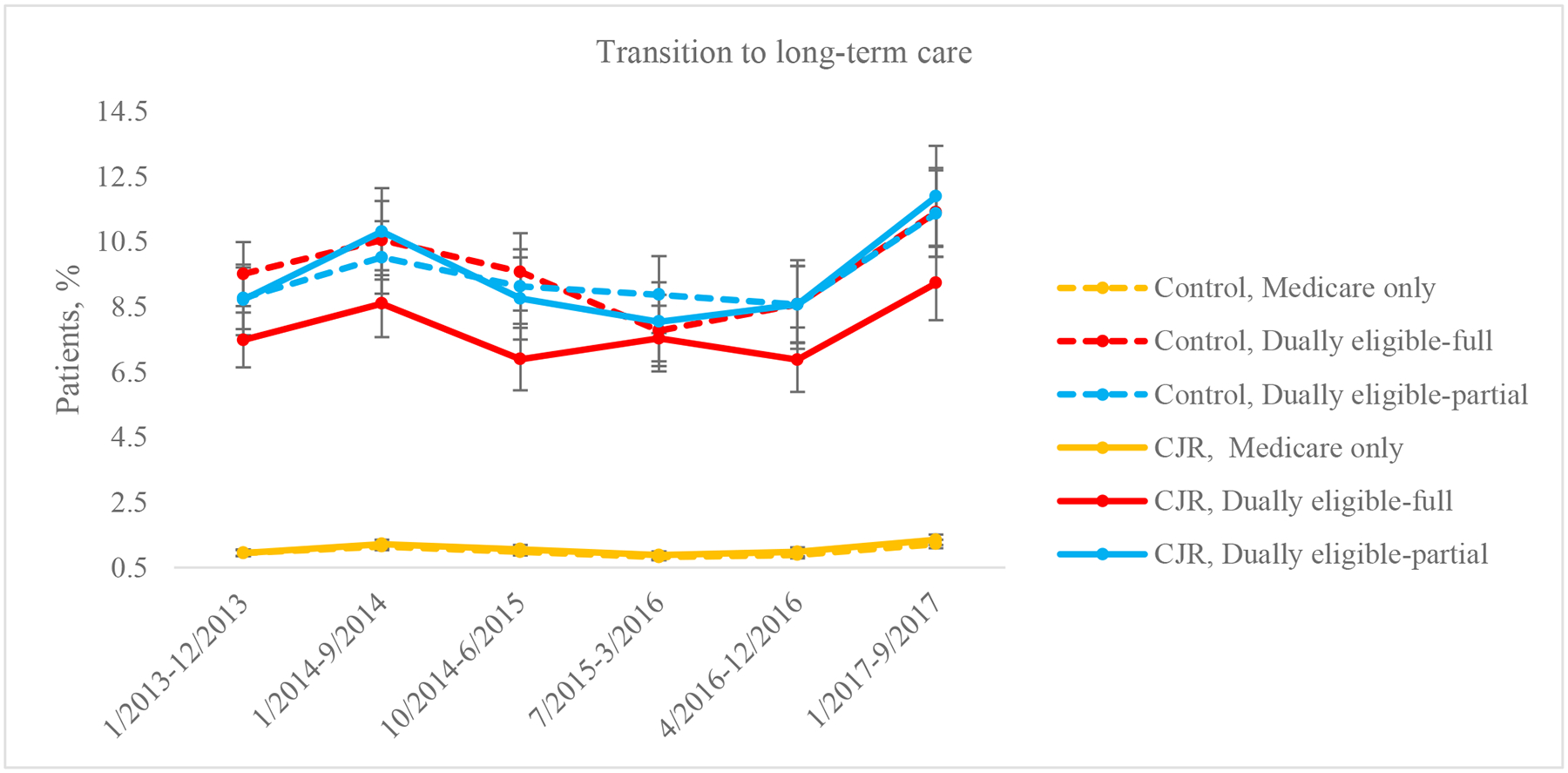
Main outcome measures: Risk-adjusted differences in rates of institutional PAC [skilled nursing facility (SNF), inpatient rehabilitation, or long-term hospital care] use and readmissions; and for the subgroup of patients discharged to SNF, risk-adjusted differences in SNF length of stay, payments, and quality measured by star ratings, rate of successful discharge to community, and rate of transition to long-stay nursing home resident.
Results: The CJR program was associated with reduced institutional PAC use and readmissions for patients in all 3 groups. For example, it was associated with reductions in 90-day readmission rate by 1.8 percentage point [DID estimate=-1.8; 95% confidence interval (CI), -2.6 to -0.9; P<0.001] for Medicare-only patients, by 1.6 percentage points (DID estimate=-1.6; 95% CI, -3.1 to -0.1; P=0.04) for full-benefit dual eligibles, and by 2.0 percentage points (DID estimate=-2.0; 95% CI, -3.6 to -0.4; P=0.01) for partial-benefit dual eligibles. These CJR-associated effects did not differ between dual eligibles (differences in above DID estimates=0.2; 95% CI, -1.4 to 1.7; P=0.81 for full-benefit patients; and -0.3; 95% CI, -1.9 to 1.3; P=0.74 for partial-benefit patients) and Medicare-only patients. Among patients discharged to SNF, the CJR program showed no effect on successful community discharge, transition to long-term care, or their persistent disparities.
Conclusions: The CJR program did not help reduce persistent disparities in readmissions or SNF-specific outcomes related to Medicare-Medicaid dual eligibility, likely due to its lack of financial incentives for reduced disparities and improved SNF outcomes.
Copyright © 2020 Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Mandatory Medicare Bundled Payment Program for Lower Extremity Joint Replacement and Discharge to Institutional Postacute Care: Interim Analysis of the First Year of a 5-Year Randomized Trial.JAMA. 2018 Sep 4;320(9):892-900. doi: 10.1001/jama.2018.12346. JAMA. 2018. PMID: 30193277 Free PMC article. Clinical Trial.
-
Association of the Mandatory Medicare Bundled Payment With Joint Replacement Outcomes in Hospitals With Disadvantaged Patients.JAMA Netw Open. 2019 Nov 1;2(11):e1914696. doi: 10.1001/jamanetworkopen.2019.14696. JAMA Netw Open. 2019. PMID: 31693127 Free PMC article.
-
Trends in Postacute Care Use and Outcomes After Hip and Knee Replacements in Dual-Eligible Medicare and Medicaid Beneficiaries, 2013-2016.JAMA Netw Open. 2020 Mar 2;3(3):e200368. doi: 10.1001/jamanetworkopen.2020.0368. JAMA Netw Open. 2020. PMID: 32129866 Free PMC article.
-
Lessons Learned From the Comprehensive Care for Joint Replacement Model at an Academic Tertiary Center: The Good, the Bad, and the Ugly.J Arthroplasty. 2023 Jul;38(7 Suppl 2):S54-S62. doi: 10.1016/j.arth.2023.02.014. Epub 2023 Feb 11. J Arthroplasty. 2023. PMID: 36781061 Free PMC article. Review.
-
Effect of Bundled Payments and Health Care Reform as Alternative Payment Models in Total Joint Arthroplasty: A Clinical Review.J Arthroplasty. 2017 Aug;32(8):2590-2597. doi: 10.1016/j.arth.2017.03.027. Epub 2017 Mar 20. J Arthroplasty. 2017. PMID: 28438453 Review.
Cited by
-
Temporal Trends in the Rate of Revision Total Knee Arthroplasty for Prosthetic Joint Infection.Arthroplast Today. 2024 Jul 3;28:101442. doi: 10.1016/j.artd.2024.101442. eCollection 2024 Aug. Arthroplast Today. 2024. PMID: 39071089 Free PMC article.
-
Beyond Discharge Disposition: A Scoping Review on Sociodemographic Disparities in Rehabilitation Use After Hip and Knee Arthroplasty.Phys Ther. 2024 Oct 2;104(10):pzae074. doi: 10.1093/ptj/pzae074. Phys Ther. 2024. PMID: 38887053 Free PMC article.
-
Effects of Maryland's All-Payer Model on elective joint replacement surgery.Am J Manag Care. 2025 May 1;31(5):e120-e124. doi: 10.37765/ajmc.2025.89735. Am J Manag Care. 2025. PMID: 40387719
-
Association of the Comprehensive Care for Joint Replacement Model With Disparities in the Use of Total Hip and Total Knee Replacement.JAMA Netw Open. 2021 May 3;4(5):e2111858. doi: 10.1001/jamanetworkopen.2021.11858. JAMA Netw Open. 2021. PMID: 34047790 Free PMC article.
-
The Effect of CMS's Comprehensive Care for Joint Replacement Bundled Payment Model on Trajectories of Post-acute Rehabilitation Care After Total Hip Arthroplasty.Arch Phys Med Rehabil. 2022 Dec;103(12):2398-2403. doi: 10.1016/j.apmr.2022.05.018. Epub 2022 Jun 26. Arch Phys Med Rehabil. 2022. PMID: 35760109 Free PMC article.
References
-
- Centers for Medicare and Medicaid Services. Comprehensive care for joint replacement model. https://goo.gl/2Xe4vN. Last updated on 01/14/2020. Accessed February 11, 2020.
-
- Joynt Maddox KE, Orav EJ, Zheng J, Epstein AM. Post-Acute Care After Joint Replacement in Medicare’s Bundled Payments for Care Improvement Initiative. J Am Geriatr Soc. 2019;67(5):1027–1035. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
