

Zuska's breast disease: Breast imaging findings and histopathologic overview
- PMID: 33273766
- PMCID: PMC7694733
- DOI: 10.4103/ijri.IJRI_207_20
Zuska's breast disease: Breast imaging findings and histopathologic overview
Abstract
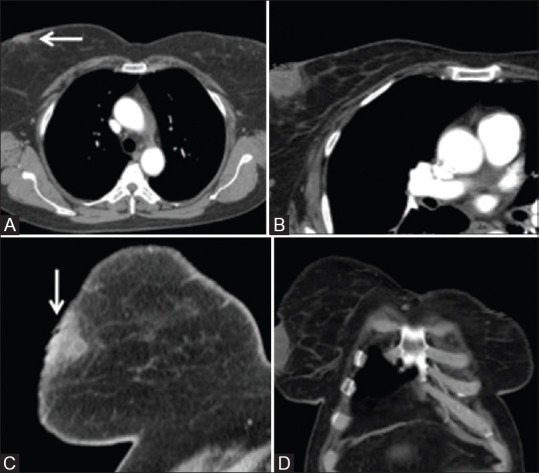
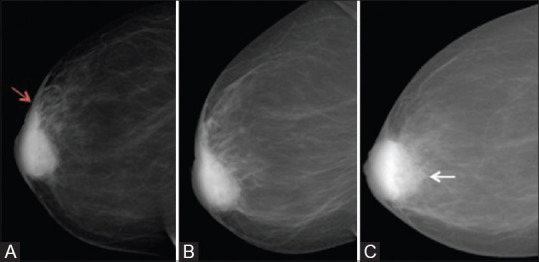
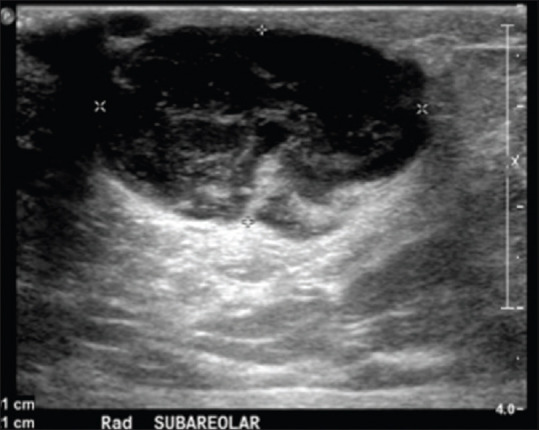
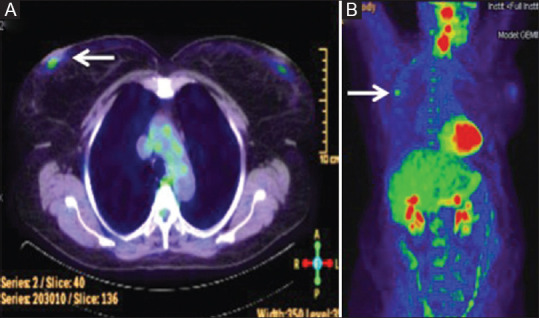
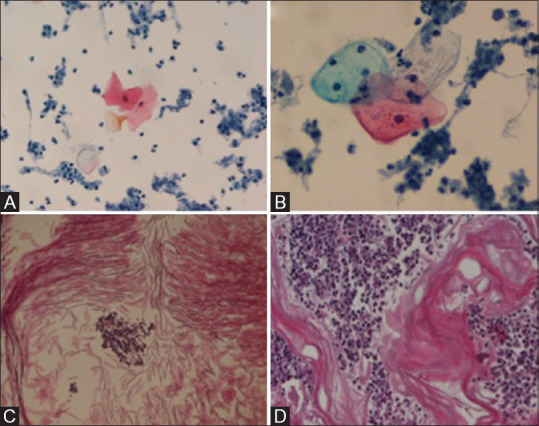
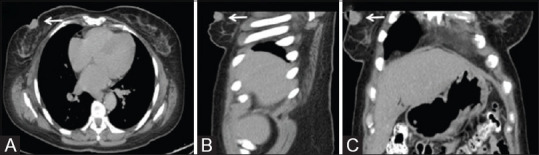
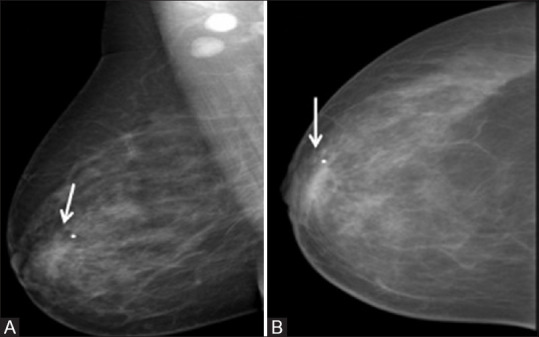
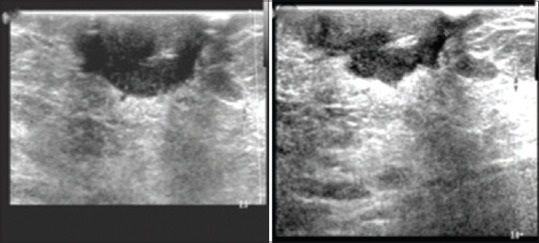
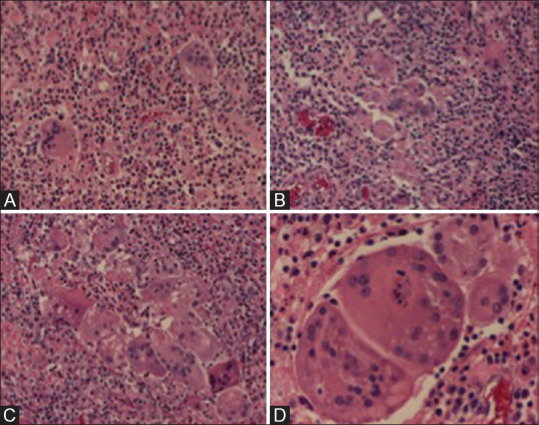
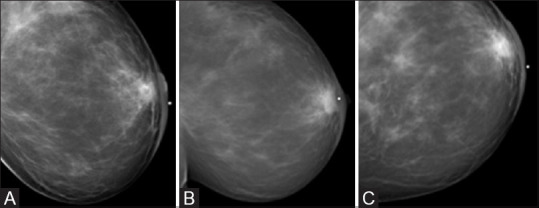
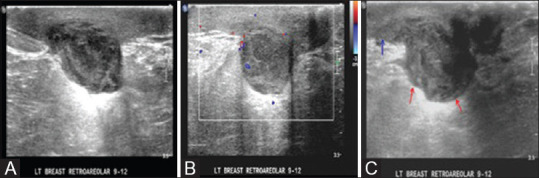
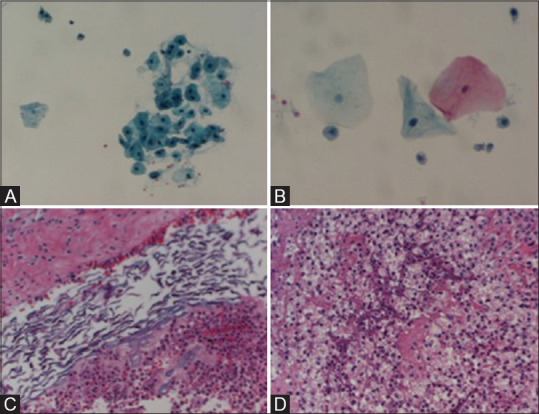
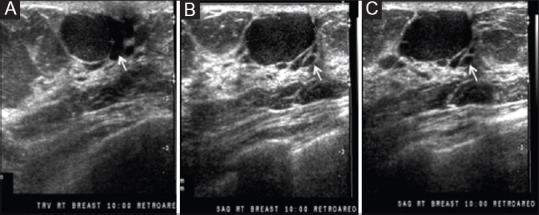
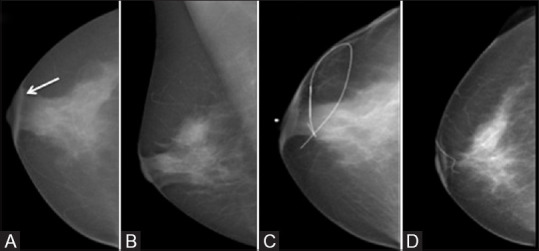
Zuska's disease describes the clinical condition of recurrent central or periareolar nonpuerperal abscesses associated with lactiferous fistulas. Pathogenesis involves the occlusion of an abnormal duct through an epithelial desquamation process that causes ductal dilatation, stasis of secretions, and periductal inflammation. Patients with Zuska's disease may develop chronic draining sinuses near the areola from lactiferous ducts fistula; therefore, the underlying abnormal duct system must be located and excised for proper treatment. Zuska's disease is often misdiagnosed and mistreated and is associated with significant morbidity, including the recurrence of abscess and cutaneous fistula formation. This case series aimed to help clinicians investigate and manage this disorder. The clinical and imaging findings, histopathologic correlation, and treatment of Zuska's disease are discussed.
Keywords: Abscess; Zuska's disease; breast diseases; lactiferous fistula.
Copyright: © 2020 Indian Journal of Radiology and Imaging.
Conflict of interest statement
There are no conflicts of interest.
Figures

References
-
- Kasales CJ, Han B, Smith JS, Chetlen AL, Kaneda HJ, Shereef S. Nonpuerperal mastitis and subareolar abscess of the breast. Am J Roentgenol. 2014;202:W133–9. - PubMed
-
- Trop I, Dugas A, Davis J, El Khoury M, Boileau JF, Larouche N, et al. Breast abscesses: Evidence-based algorithms for diagnosis, management, and follow-up. Radiographics. 2011;31:1683–99. - PubMed
-
- Zuska JJ, Crile G, Ayres WW. Fistulas of lactifierous ducts. Am J Surg. 1951;81:312–7. - PubMed
-
- Gollapalli V, Liao J, Dudakovic A, Sugg SL, Scott-Conner CE, Weigel RJ. Risk factors for development and recurrence of primary breast abscesses. J Am Coll Surg. 2010;211:41–8. - PubMed
LinkOut - more resources
Full Text Sources