

Management of Osteogenesis Imperfecta: A Multidisciplinary Comprehensive Approach
- PMID: 33274017
- PMCID: PMC7683189
- DOI: 10.4055/cios20060
Management of Osteogenesis Imperfecta: A Multidisciplinary Comprehensive Approach
Abstract
Osteogenesis imperfecta (OI) is characterized by recurring fractures and limb and spine deformities. With the advent of medical therapeutics and the discovery of causative genes, as well as the introduction of a newly devised intramedullary rod, the general condition and ambulatory function of patients diagnosed with OI have been improved over the past decades. This review covers recent developments in research and management of OI.
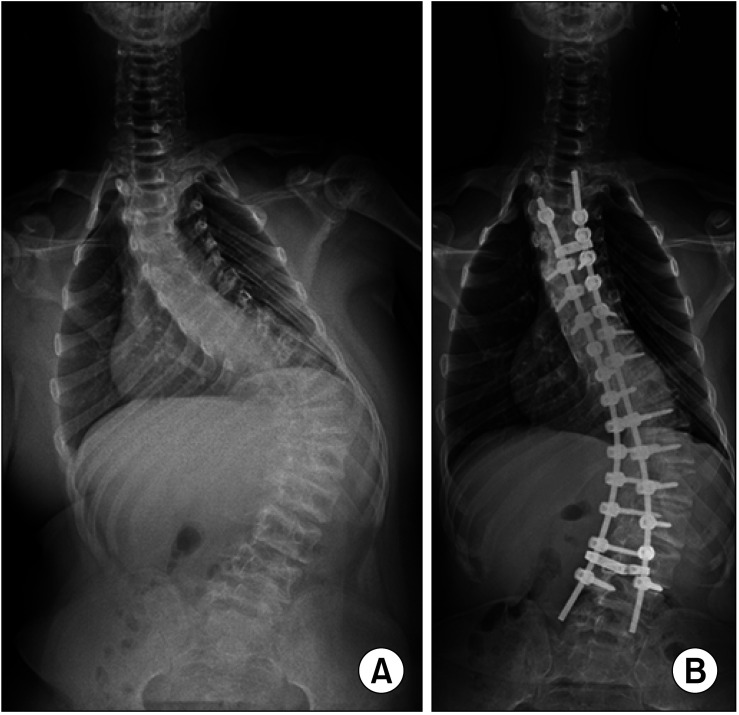
Keywords: Bisphosphonate; Gene; Intramedullary nailing; Osteogenesis imperfecta; Scoliosis.
Copyright © 2020 by The Korean Orthopaedic Association.
Conflict of interest statement
CONFLICT OF INTEREST: No potential conflict of interest relevant to this article was reported.
Figures

References
-
- Mortier GR, Cohn DH, Cormier-Daire V, et al. Nosology and classification of genetic skeletal disorders: 2019 revision. Am J Med Genet A. 2019;179(12):2393–2419. - PubMed
-
- Trejo P, Palomo T, Montpetit K, et al. Long-term follow-up in osteogenesis imperfecta type VI. Osteoporos Int. 2017;28(10):2975–2983. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
