

Effect of Platelet-Rich Plasma Injection on Mild or Moderate Carpal Tunnel Syndrome: An Updated Systematic Review and Meta-Analysis of Randomized Controlled Trials
- PMID: 33274213
- PMCID: PMC7683131
- DOI: 10.1155/2020/5089378
Effect of Platelet-Rich Plasma Injection on Mild or Moderate Carpal Tunnel Syndrome: An Updated Systematic Review and Meta-Analysis of Randomized Controlled Trials
Abstract
Objective: To evaluate efficacy of platelet-rich plasma (PRP) injection in carpal tunnel syndrome (CTS), we conducted this meta-analysis, as well as proposed a protocol for its application in curative processes.
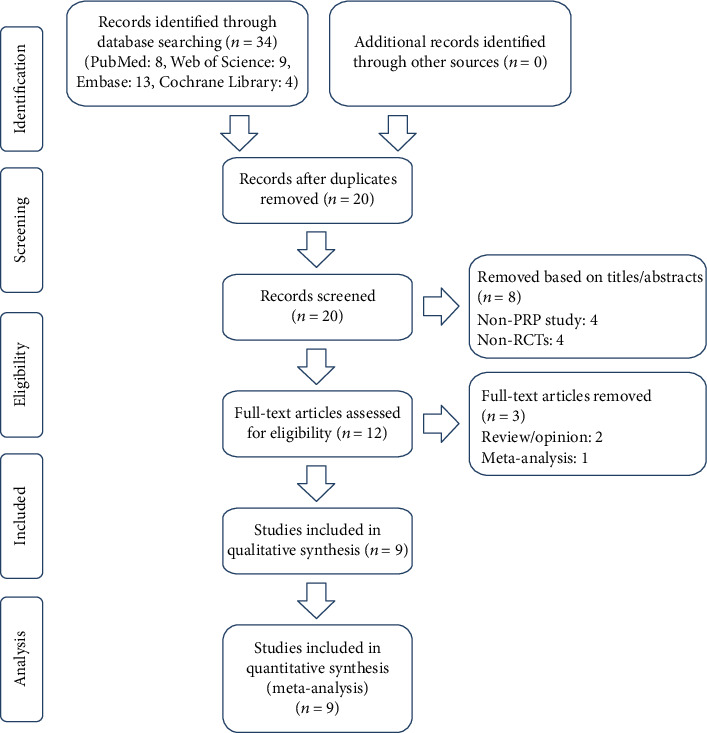
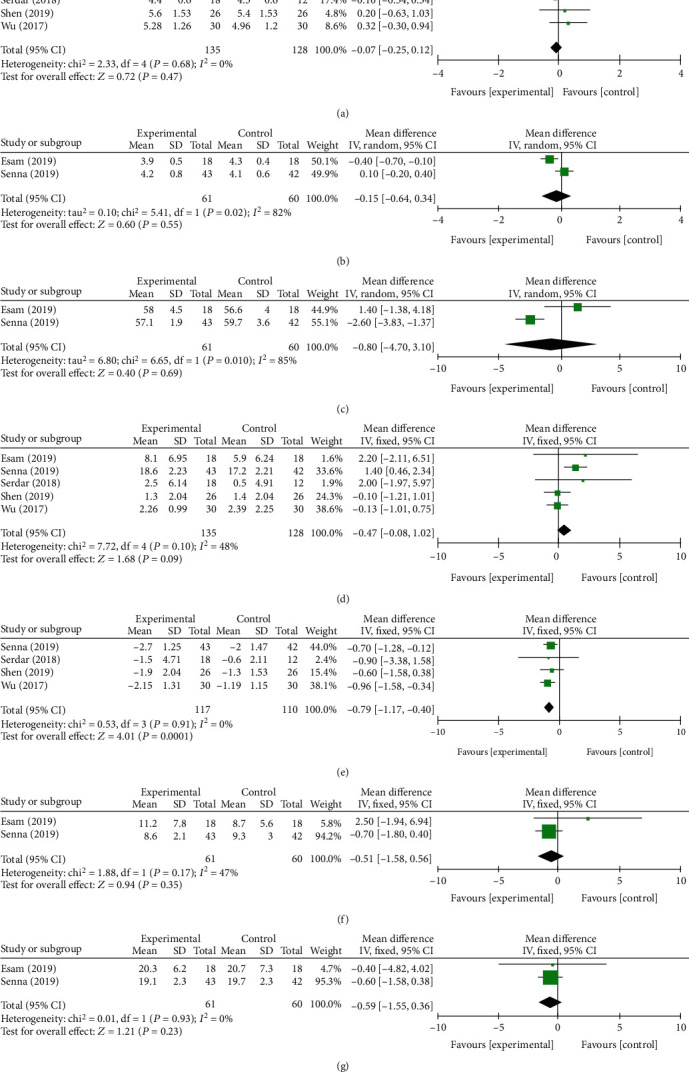
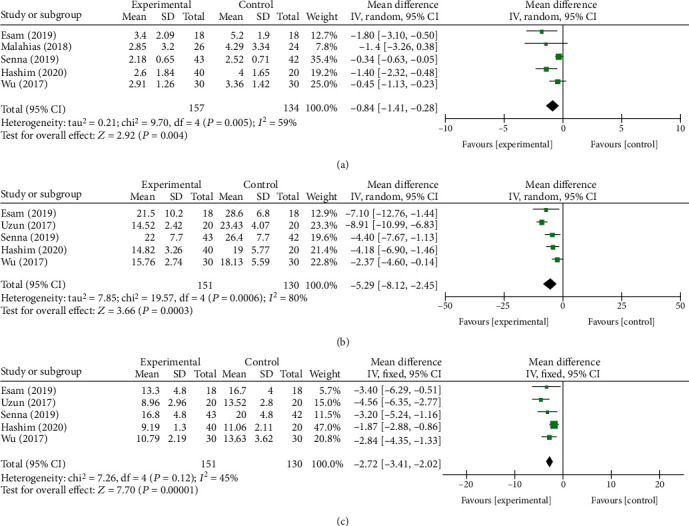
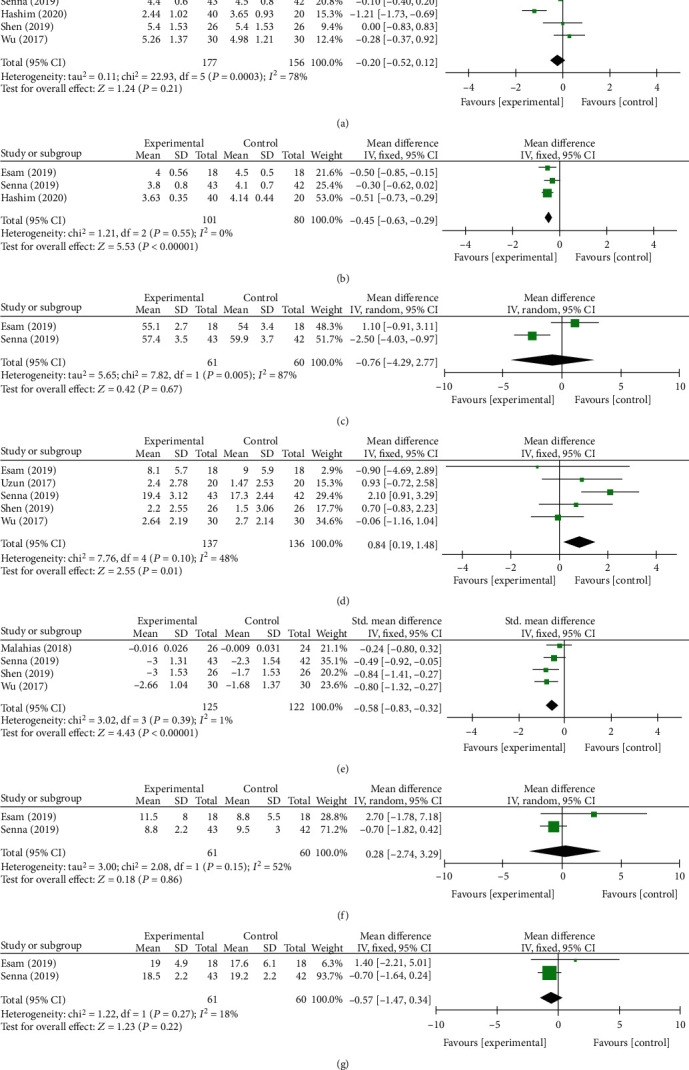
Methods: All randomized controlled trials (RCTs) of PRP for the management of mild or moderate CTS were included in this study. Database search was conducted from study inception to July 2020, including PubMed, Embase, Web of Science, and Cochrane Library. We used visual analogue scores (VAS) and the Boston Carpal Tunnel Questionnaire (BCTQ) as evaluation tools for primary outcomes. Second outcomes comprised cross-sectional area (ΔCSA) and electrophysiological indexes including distal motor latency (DML), sensory peak latency (SPL), motor nerve conduction velocity (MNCV), sensory nerve conduction velocity (SNCV), compound muscle action potential (CMAP), and sensory nerve action potential (SNAP). The pooled data were analyzed using RevMan 5.3. Subgroup and sensitivity analyses were conducted with the evidence of heterogeneity. Egger' test was used to investigate publication bias.
Results: 9 RCTs were finally screened out with 434 patients included. Control groups comprised corticosteroid injection in 5 trials, saline injection in 1 trial, and splint in 3 trials. At the 1st month after follow-up, only ΔCSA between the PRP group and the control group showed significant difference (P < 0.05). In the 3rd month, there were statistically significant differences in VAS, BCTQ, SPL, SNCV, and ΔCSA between two groups (P < 0.05), while no statistically significant differences were found in the remaining outcomes. In the 6th month, there were statistically significant differences at BCTQ (P < 0.05) in primary outcomes and ΔCSA (P < 0.05) in secondary outcomes between two groups. As to adverse events in PRP injection, only one study reported increased pain sensation within 48 h after injections.
Conclusion: This systematic review and meta-analysis demonstrates that the PRP could be effective for mild to moderate CTS and superior to traditional conservative treatments in improving pain and function and reducing the swelling of the median nerve for a mid-long-term effect. To some extent, the electrophysiological indexes also improved after PRP injection compared with others conservative treatments.
Copyright © 2020 Chunke Dong et al.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures






References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
