

Childhood Neurotoxicity and Brain Resilience to Adverse Events during Adulthood
- PMID: 33274777
- PMCID: PMC7897299
- DOI: 10.1002/ana.25981
Childhood Neurotoxicity and Brain Resilience to Adverse Events during Adulthood
Abstract
Objective: This study used childhood cancer survivors as a novel model to study whether children who experience central nervous system (CNS) injury are at higher risk for neurocognitive impairment associated with subsequent late onset chronic health conditions (CHCs).
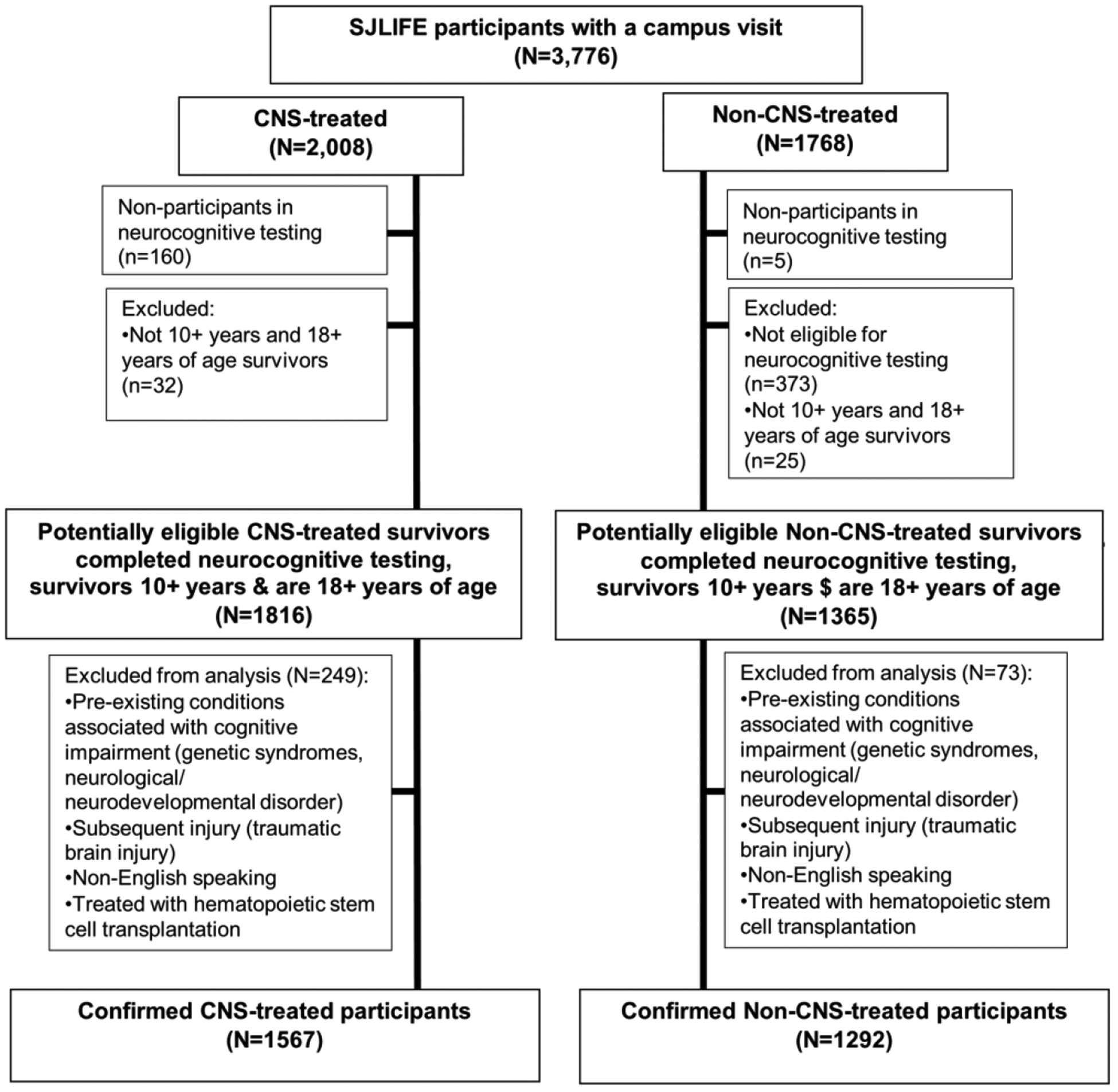
Methods: Adult survivors of childhood cancer (n = 2,859, ≥10 years from diagnosis, ≥18 years old) completed a comprehensive neurocognitive battery and clinical examination. Neurocognitive impairment was defined as age-adjusted z score < 10th percentile. Participants impaired on ≥3 tests had global impairment. CHCs were graded using the Common Terminology Criteria for Adverse Events v4.3 (grade 1, mild; 2, moderate; 3, severe/disabling; 4, life-threatening) and were combined into a severity/burden score by frequency and grade (none/low, medium, high, and very high). A total of 1,598 survivors received CNS-directed therapy including cranial radiation, intrathecal methotrexate, or neurosurgery. Logistic regression estimated the odds of neurocognitive impairment associated with severity/burden score and grade 2 to 4 conditions, stratified by CNS treatment.
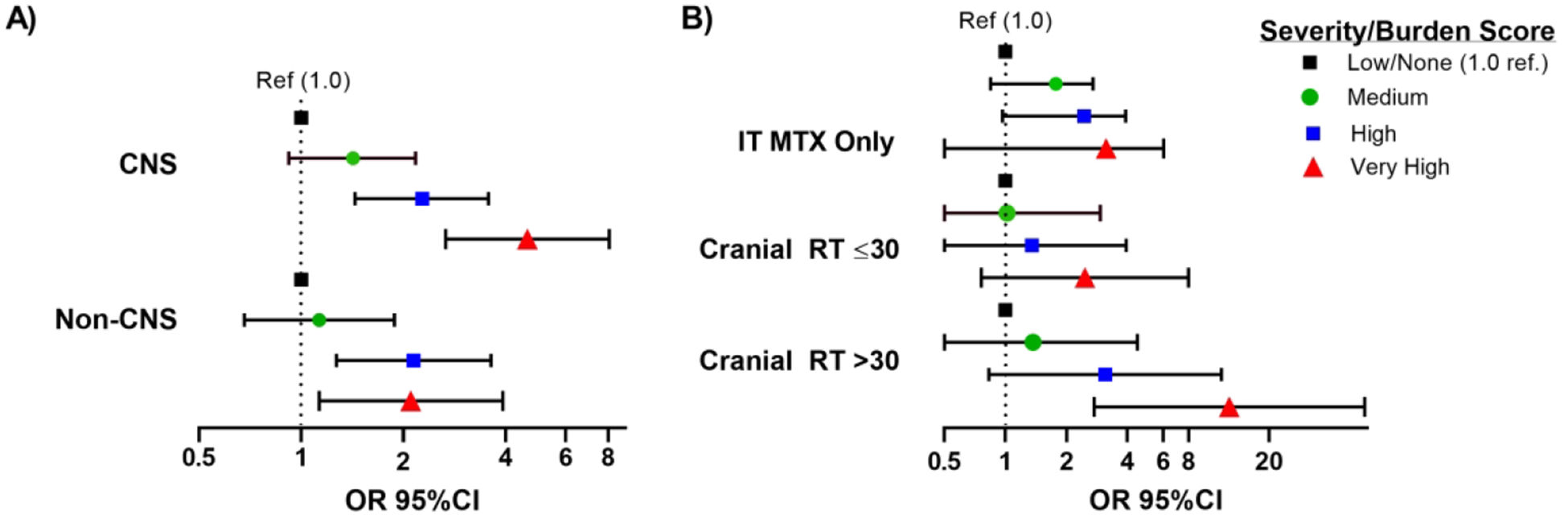
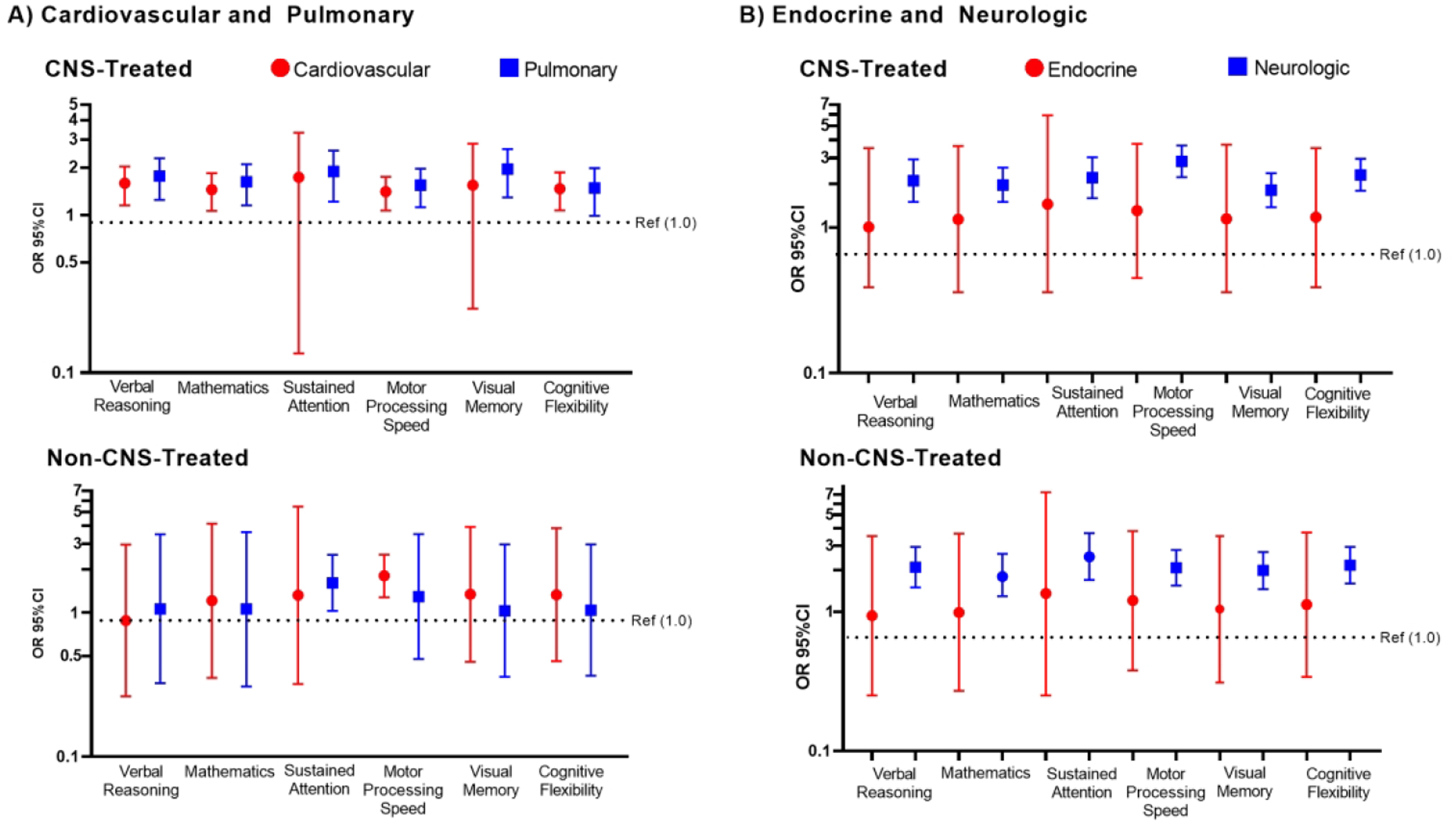
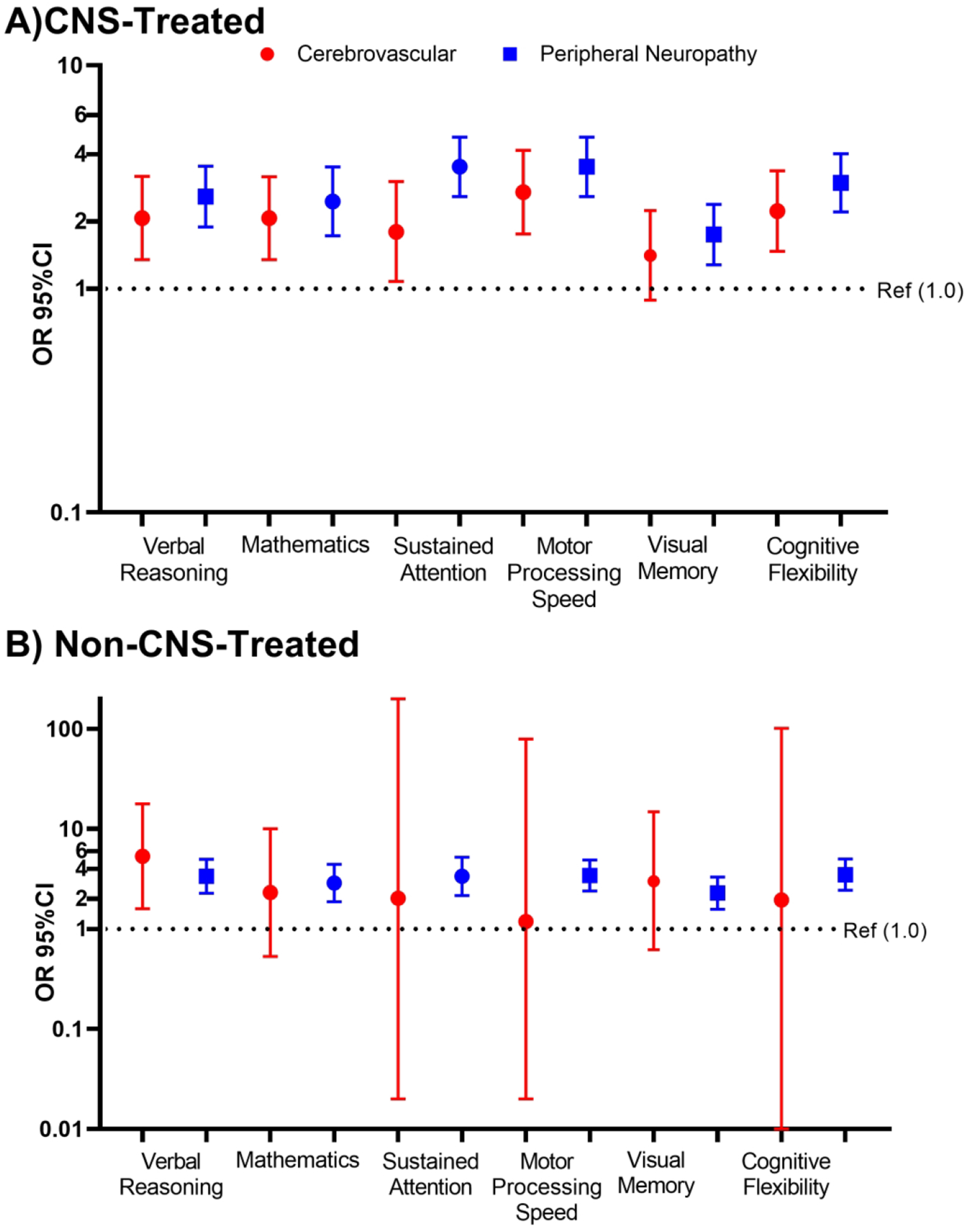
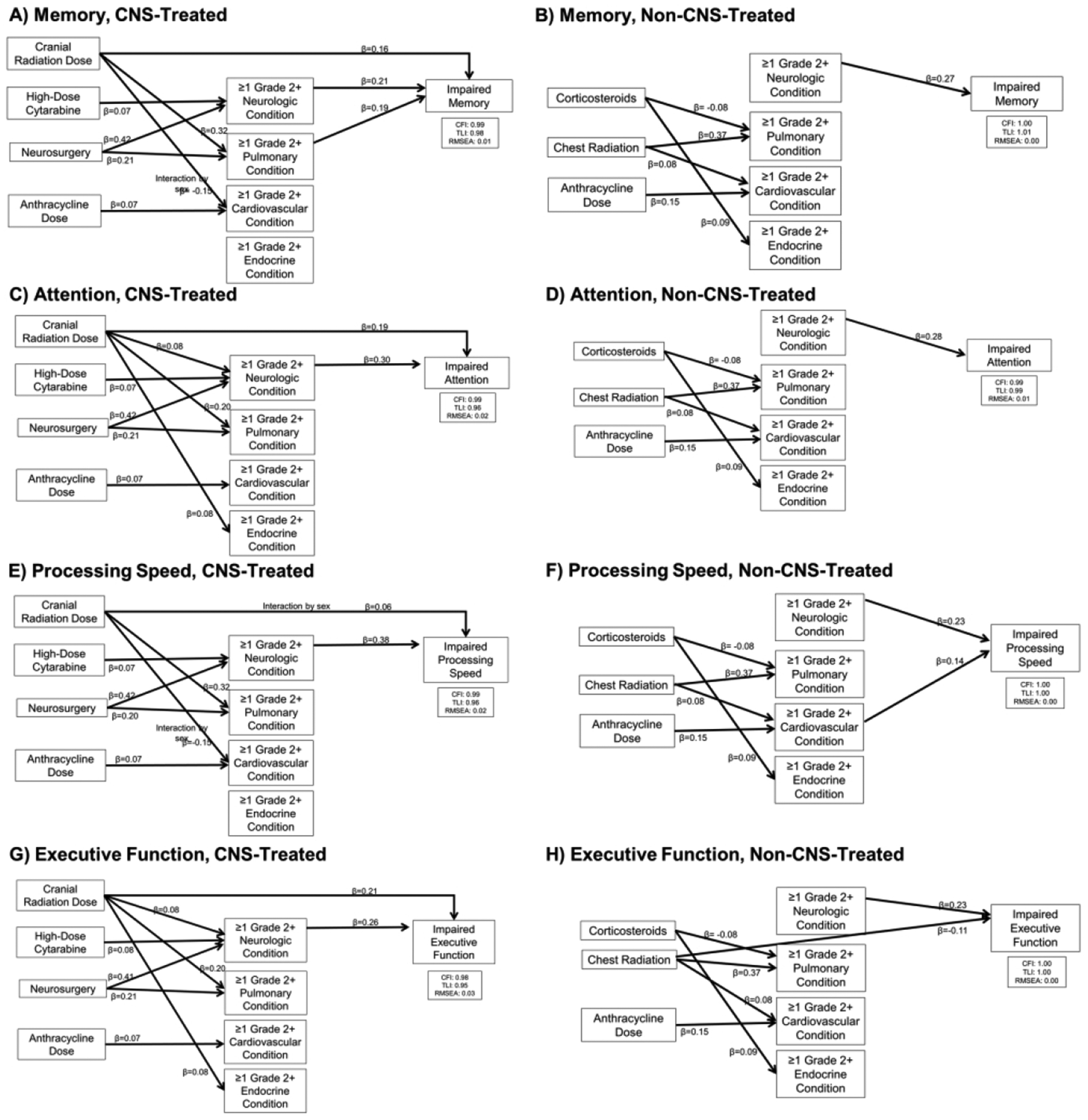
Results: CNS-treated survivors performed worse than non-CNS-treated survivors on all neurocognitive tests and were more likely to have global neurocognitive impairment (46.9% vs 35.3%, p < 0.001). After adjusting for demographic and treatment factors, there was a dose-response association between severity/burden score and global neurocognitive impairment, but only among CNS-treated survivors (high odds ratio [OR] = 2.24, 95% confidence interval [CI] = 1.42-3.53; very high OR = 4.07, 95% CI = 2.30-7.17). Cardiovascular and pulmonary conditions were associated with processing speed, executive function, and memory impairments in CNS-treated but not non-CNS-treated survivors who were impacted by neurologic conditions.
Interpretation: Reduced cognitive/brain reserve associated with CNS-directed therapy during childhood may make survivors vulnerable to adverse cognitive effects of cardiopulmonary conditions during adulthood. ANN NEUROL 2021;89:534-545.
© 2020 American Neurological Association.
Conflict of interest statement
Potential Conflicts of Interest
The authors declare no conflicts of interest.
Figures
References
-
- Stern Y, Gurland B, Tatemichi TK, Tang MX, Wilder D, Mayeux R. Influence of education and occupation on the incidence of Alzheimer’s disease. Jama. 1994. April 6;271(13):1004–10. - PubMed
-
- Sumowski JF, Chiaravalloti N, DeLuca J. Cognitive reserve protects against cognitive dysfunction in multiple sclerosis. J Clin Exp Neuropsychol. 2009. November;31(8):913–26. - PubMed
-
- Poletti M, Emre M, Bonuccelli U. Mild cognitive impairment and cognitive reserve in Parkinson’s disease. Parkinsonism Relat Disord. 2011. September;17(8):579–86. - PubMed
-
- Xu W, Tan L, Wang HF, et al. Education and Risk of Dementia: Dose-Response Meta-Analysis of Prospective Cohort Studies. Mol Neurobiol. 2016. July;53(5):3113–23. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
