

Prostate Radiotherapy With Adjuvant Androgen Deprivation Therapy (ADT) Improves Metastasis-Free Survival Compared to Neoadjuvant ADT: An Individual Patient Meta-Analysis
- PMID: 33275486
- PMCID: PMC8189640
- DOI: 10.1200/JCO.20.02438
Prostate Radiotherapy With Adjuvant Androgen Deprivation Therapy (ADT) Improves Metastasis-Free Survival Compared to Neoadjuvant ADT: An Individual Patient Meta-Analysis
Abstract
Purpose: There remains a lack of clarity regarding the influence of sequencing of androgen deprivation therapy (ADT) and radiotherapy (RT) on outcomes in prostate cancer (PCa). Herein, we evaluate the optimal sequencing of ADT with prostate-directed RT in localized PCa.
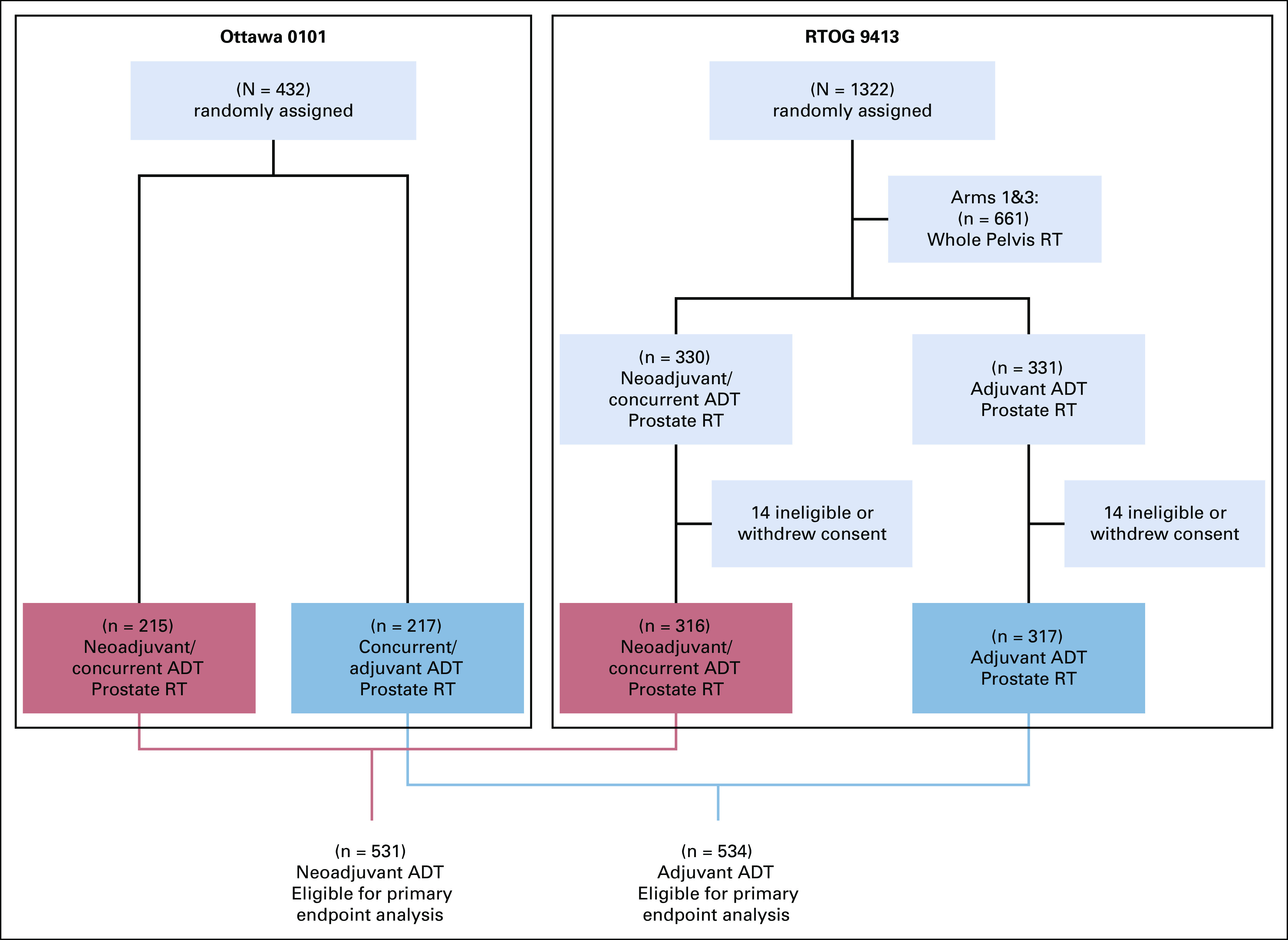
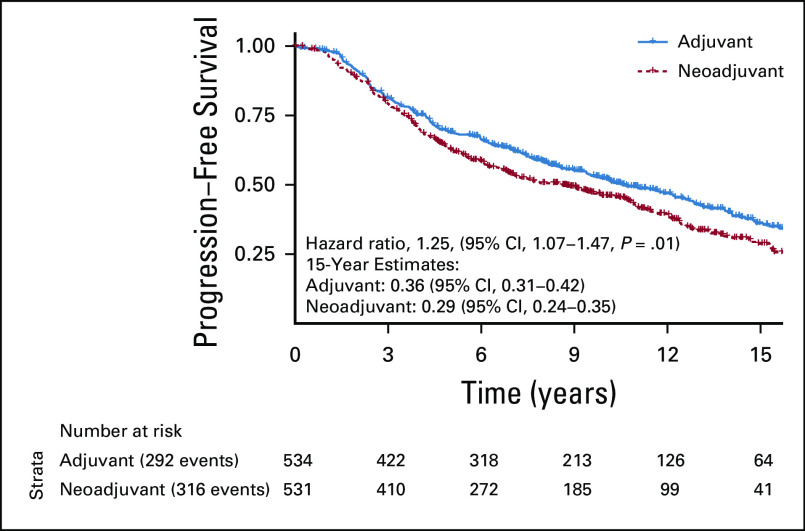
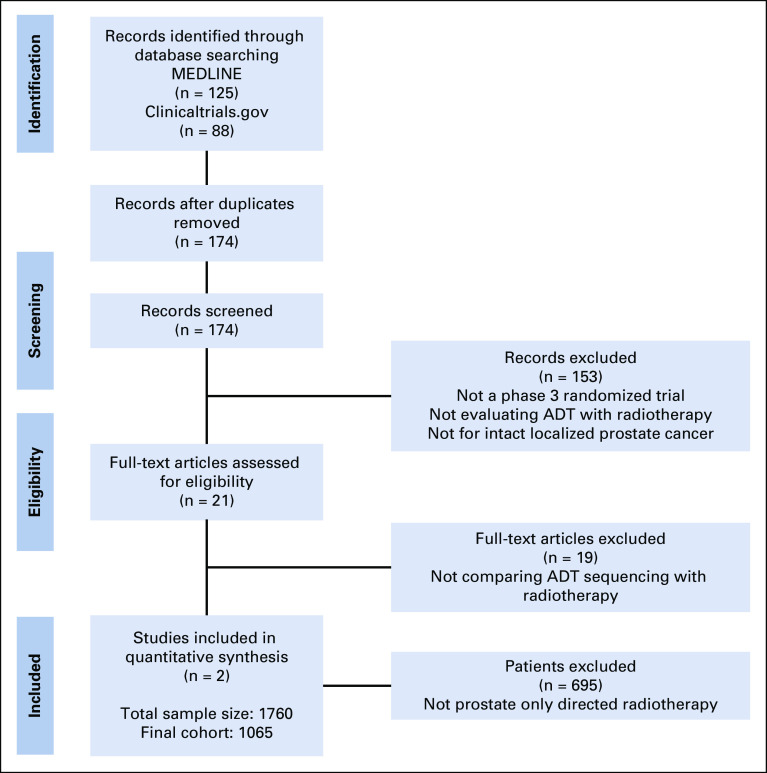
Methods: MEDLINE (1966-2018), Embase (1982-2018), ClinicalTrials.gov, and conference proceedings (1990-2018) were searched to identify randomized trials evaluating the sequencing, but not duration, of ADT with RT. Two randomized phase III trials were identified, and individual patient data were obtained: Ottawa 0101 and NRG Oncology's Radiation Therapy Oncology Group 9413. Ottawa 0101 randomly assigned patients to neoadjuvant or concurrent versus concurrent or adjuvant short-term ADT. Radiation Therapy Oncology Group 9413, a 2 × 2 factorial trial, included a random assignment of neoadjuvant or concurrent versus adjuvant short-term ADT. The neoadjuvant or concurrent ADT arms of both trials were combined into the neoadjuvant group, and the arms receiving adjuvant ADT were combined into the adjuvant group. The primary end point of this meta-analysis was progression-free survival (PFS).
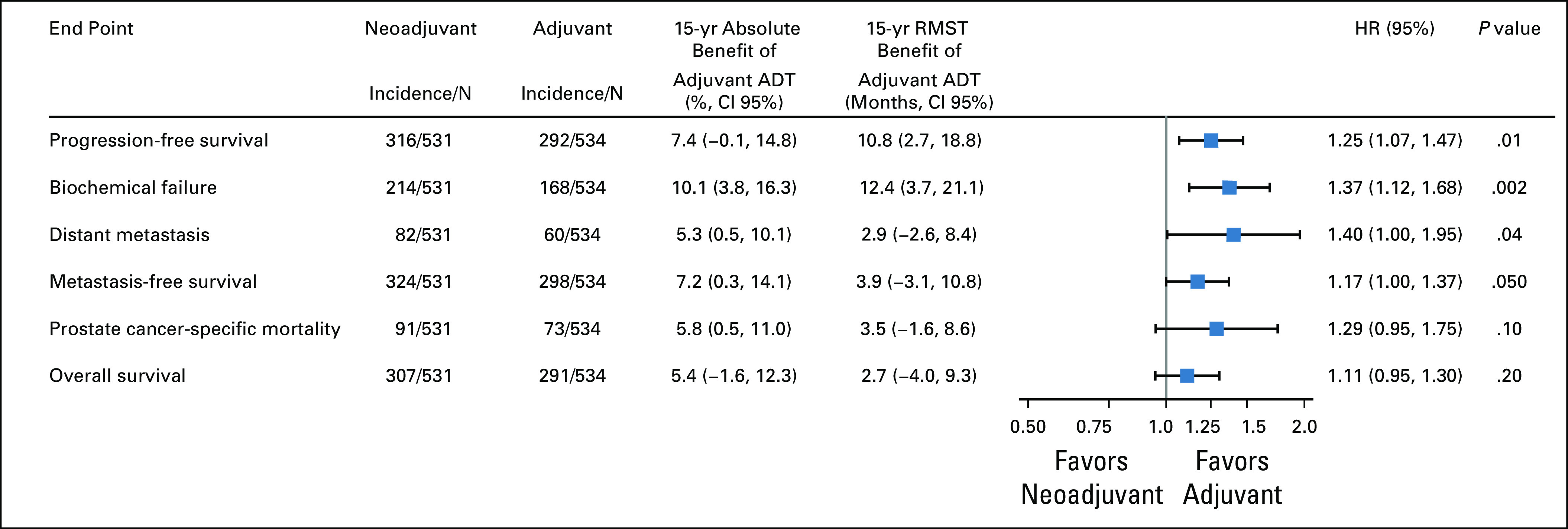
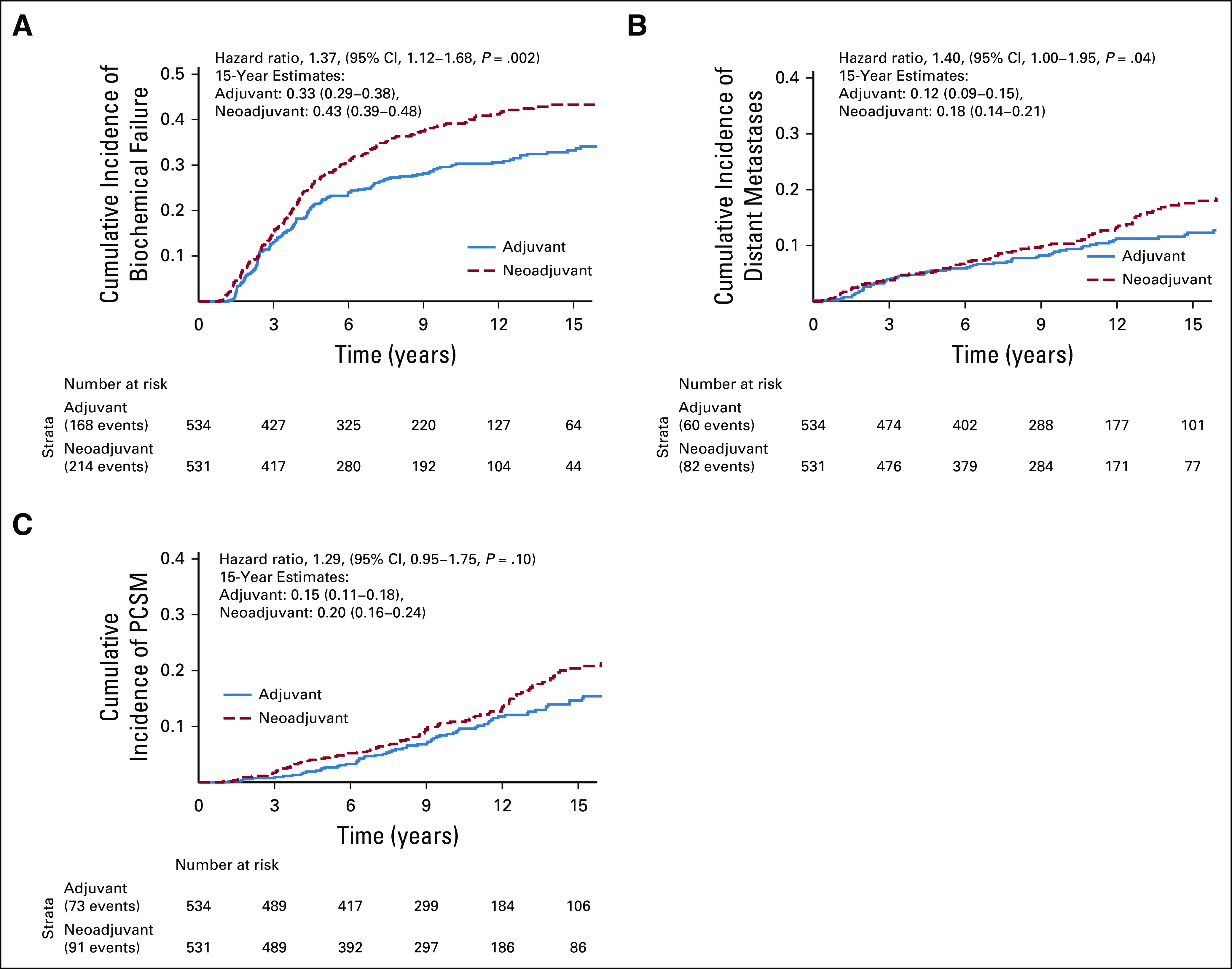
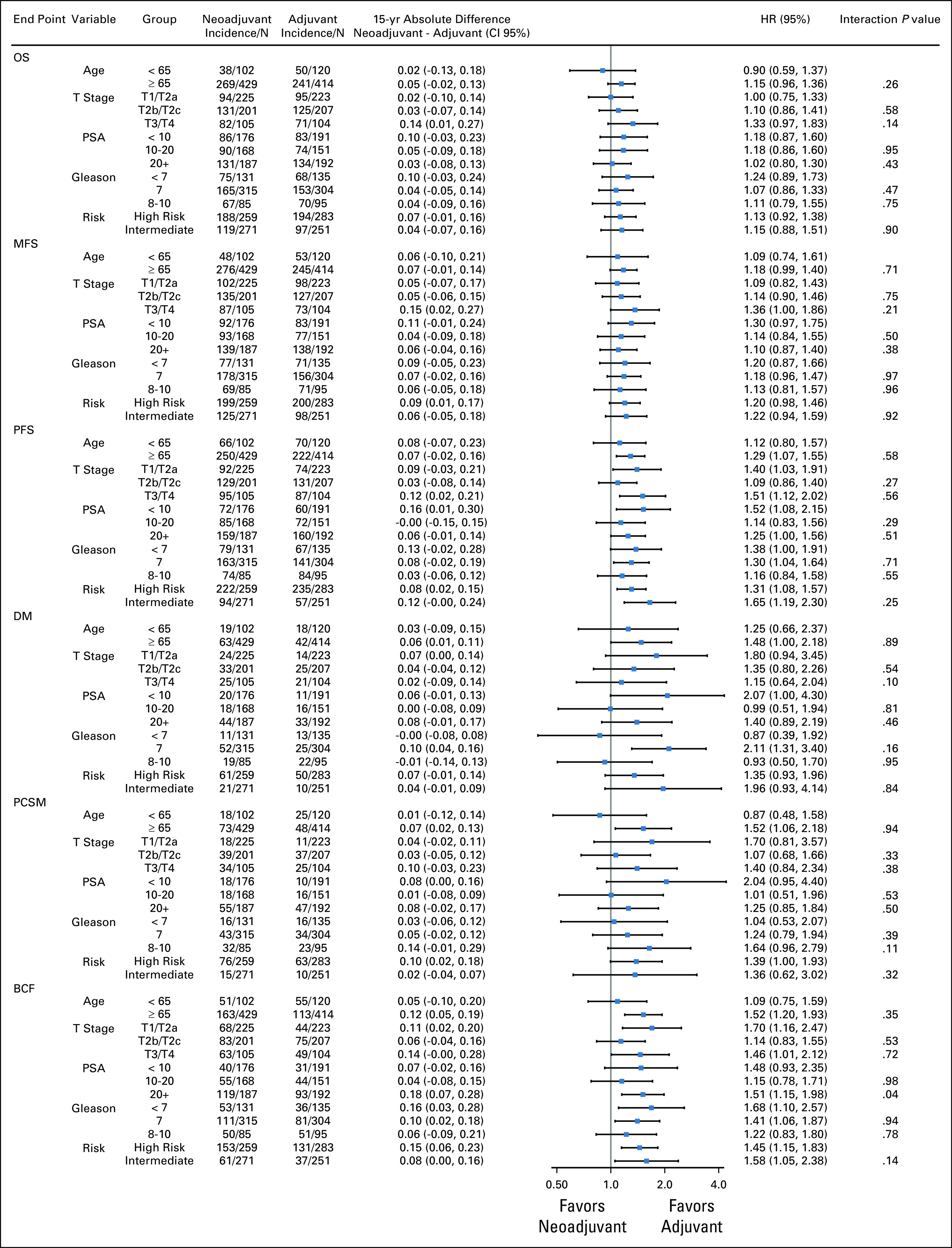
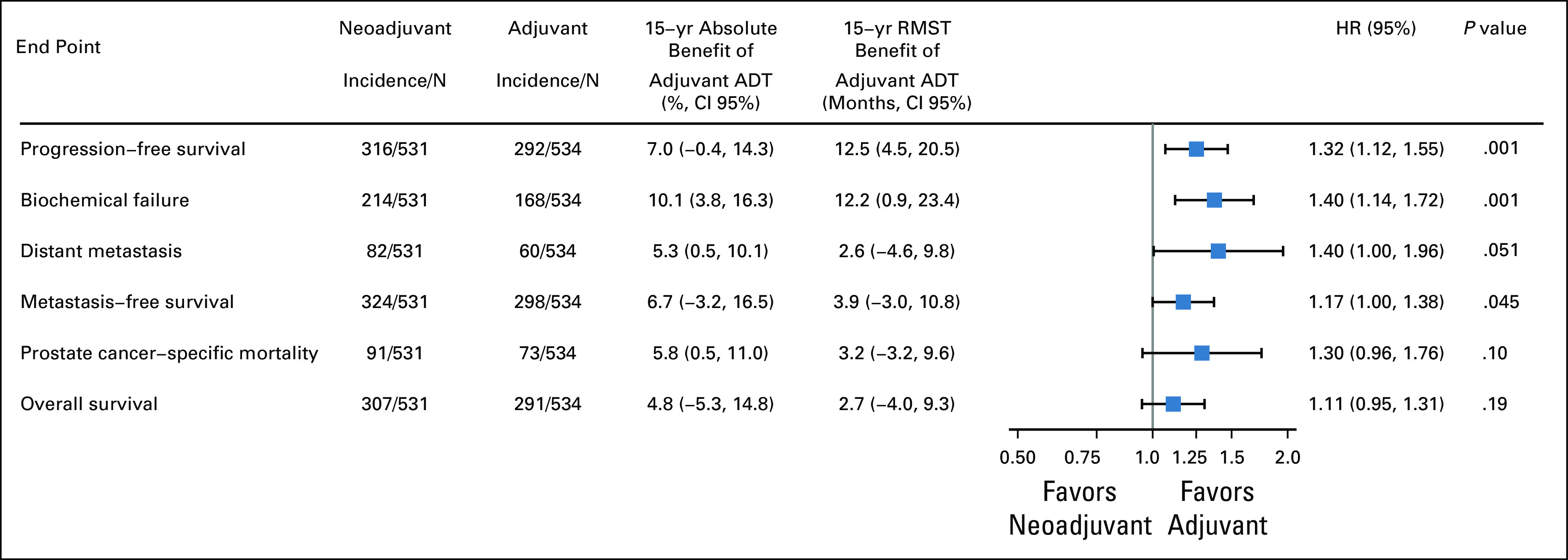
Results: The median follow-up was 14.9 years. Overall, 1,065 patients were included (531 neoadjuvant and 534 adjuvant). PFS was significantly improved in the adjuvant group (15-year PFS, 29% v 36%, hazard ratio [HR], 1.25 [95% CI, 1.07 to 1.47], P = .01). Biochemical failure (subdistribution HR [sHR], 1.37 [95% CI, 1.12 to 1.68], P = .002), distant metastasis (sHR, 1.40 [95% CI, 1.00 to 1.95], P = .04), and metastasis-free survival (HR, 1.17 [95% CI, 1.00 to 1.37], P = .050) were all significantly improved in the adjuvant group. There were no differences in late grade ≥ 3 gastrointestinal (2% v 3%, P = .33) or genitourinary toxicity (5% v 5%, P = .76) between groups.
Conclusion: The sequencing of ADT with prostate-directed RT has significant association with long-term PFS and MFS in localized PCa. Our findings favor use of an adjuvant over a neoadjuvant approach, without any increase in long-term toxicity.
Trial registration: ClinicalTrials.gov NCT00769548.
Figures
Comment in
-
Reply to S. Sundar et al and S. Höcht et al.J Clin Oncol. 2021 Jul 10;39(20):2316-2317. doi: 10.1200/JCO.21.00411. Epub 2021 Apr 29. J Clin Oncol. 2021. PMID: 33914593 No abstract available.
-
Adjuvant Hormone Therapy After Prostate Radiation: Is This Data Torture?J Clin Oncol. 2021 Jul 10;39(20):2314-2315. doi: 10.1200/JCO.21.00013. Epub 2021 Apr 29. J Clin Oncol. 2021. PMID: 33914596 No abstract available.
-
Timing of ADT in Radiotherapy of Prostate Cancer.J Clin Oncol. 2021 Jul 10;39(20):2315-2316. doi: 10.1200/JCO.21.00032. Epub 2021 Apr 29. J Clin Oncol. 2021. PMID: 33914597 No abstract available.
References
-
- Pignon JP, Le Maitre A, Maillard E, et al. : Meta-analysis of chemotherapy in head and neck cancer (MACH-NC): An update on 93 randomised trials and 17,346 patients. Radiother Oncol 92:4-14, 2009 - PubMed
-
- Auperin A, Le Pechoux C, Pignon J, et al. : Concomitant radio-chemotherapy based on platin compounds in patients with locally advanced non-small cell lung cancer (NSCLC): A meta-analysis of individual data from 1764 patients. Ann Oncol 17:473-483, 2006 - PubMed
-
- Jones C, Pugh S, Sandler H, et al. : Long-term update of NRG Oncology RTOG 94-08. Int J Radiat Oncol Biol Phys 102:S31-S32, 2018
-
- Stupp R, Mason WP, Van Den Bent MJ, et al. : Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med 352:987-996, 2005 - PubMed
-
- James ND, Hussain SA, Hall E, et al. : Radiotherapy with or without chemotherapy in muscle-invasive bladder cancer. N Engl J Med 366:1477-1488, 2012 - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
