

Determining generalizability of the Canadian Kidney Cancer information system (CKCis) to the entire Canadian kidney cancer population
- PMID: 33275557
- PMCID: PMC7716824
- DOI: 10.5489/cuaj.6716
Determining generalizability of the Canadian Kidney Cancer information system (CKCis) to the entire Canadian kidney cancer population
Abstract
Introduction: The Canadian Kidney Cancer information system (CKCis) has prospectively collected data on patients with renal tumors since January 1, 2011 from 16 sites within 14 academic centers in six provinces. Canadian kidney cancer experts have used CKCis data to address several research questions. The goal of this study was to determine if the CKCis cohort is representative of the entire Canadian kidney cancer population, specifically regarding demographic and geographic distributions.
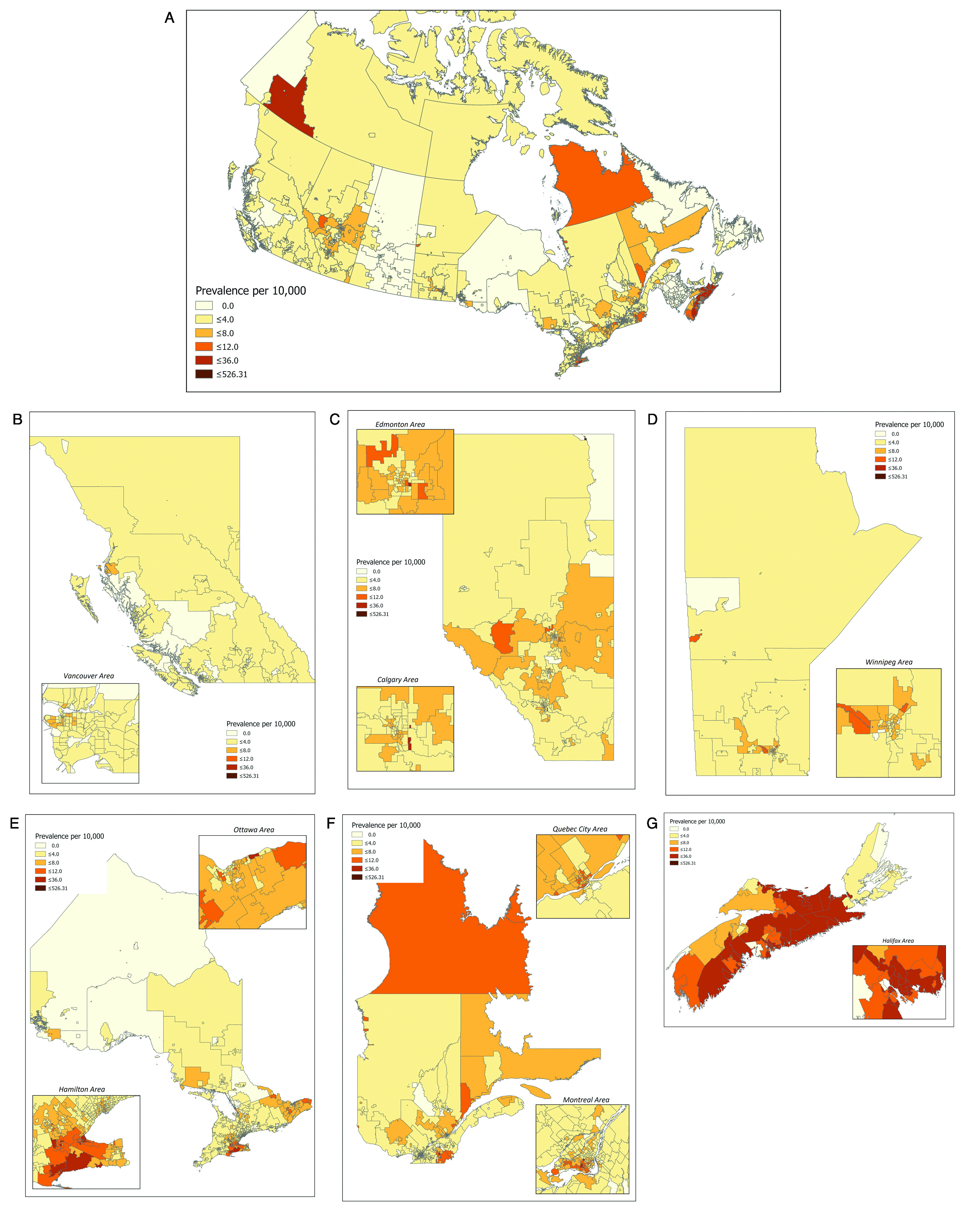
Methods: The CKCis prospective cohort was analyzed up to December 31, 2018. Baseline demographics and tumor characteristics were analyzed, including location of patients' residence at the time of CKCis entry. Geographic data is presented by province, rural vs. urban via postal code information (2nd digit=0) and by Canadian urban boundary files. To determine the proportion of renal cell carcinoma (RCC) patients that CKCis captures, CKCis accruals were compared to projected Canadian Cancer Society RCC incidence in 2016-2017 and the incidence from the 2016 Canadian Cancer Registry. To determine if the CKCis baseline data is representative, it was compared to registry data and other published data when registry data was not available.
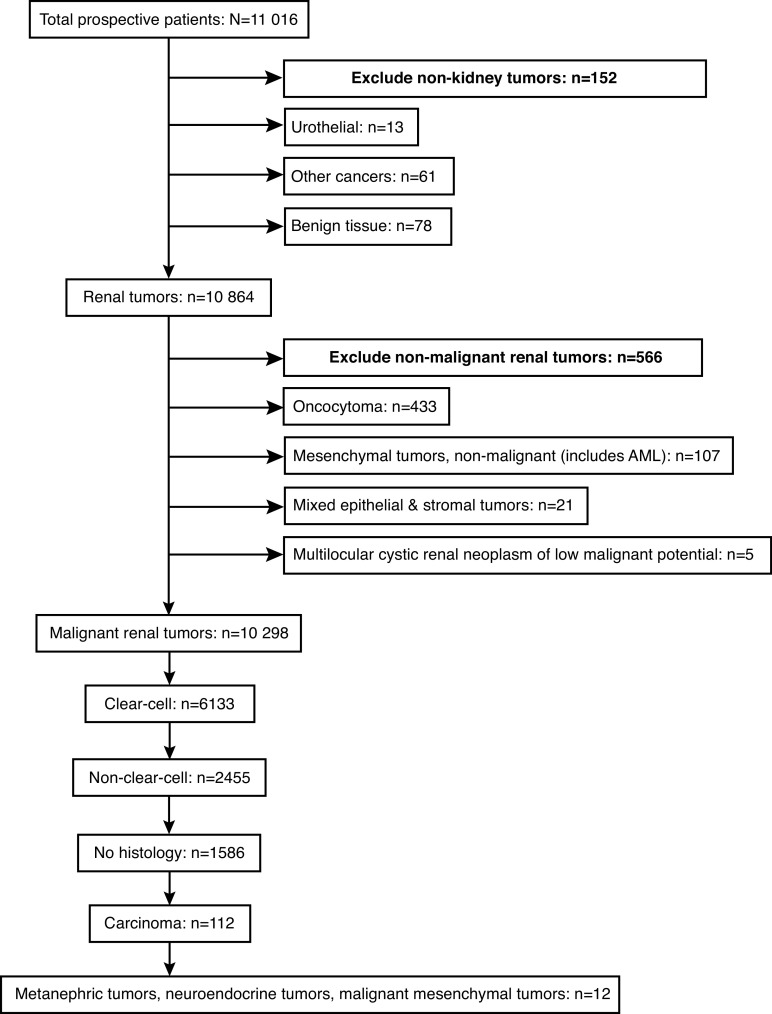
Results: This CKCis cohort includes 10 298 eligible patients: 66.6% male, median age 62.6 years; 14.6% had metastatic disease at the time of diagnosis and 70.4% had clear-cell carcinomas. The CKCis cohort captures about 1250 patients per year, which represents approximately 20% of the total kidney cancer incidence. The proportion of patients captured per province did vary from 13-43%. Rural patients make up 17% of patients, with some baseline differences between rural and urban patients. There appears to be no major differences between CKCis patient demographics and disease characteristics compared to national data sources. Canadian heat maps detailing patient location are presented.
Conclusions: CKCis contains prospective data on >10 000 Canadian kidney cancer patients, making it a valuable resource for kidney cancer research. The baseline demographic and geographic data do appear to include a broad cross-section of patients and seem to be highly representative of the Canadian kidney cancer population. Moving forward, future projects will include determining if CKCis cancer outcomes are also representative of the entire Canadian kidney cancer population and studying variations across provinces and within rural vs. urban areas.
Conflict of interest statement
Figures
References
-
- Statistics Canada. Dictionary, Census of Population. 2016. [Accessed March 6, 2020]. Available at: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310011101.
-
- Canadian Cancer Society’s Advisory Committee on Cancer Statistics. Canadian Cancer Statistics. 2015. [Accessed Jan 2, 2020]. Available at: https://www.cancer.ca/~/media/cancer.ca/CW/cancer%20information/cancer%2....
-
- Canadian Cancer Society’s Advisory Committee on Cancer Statistics. Canadian Cancer Statistics. 2016. [Accessed Jan 2, 2020]. Available at: https://www.cancer.ca/~/media/cancer.ca/CW/cancer%20information/cancer%2....
-
- Canadian Cancer Society’s Advisory Committee on Cancer Statistics. Canadian Cancer Statistics. 2017. [Accessed Jan 9, 2020]. Available at: https://www.cancer.ca/~/media/cancer.ca/CW/cancer%20information/cancer%2....
-
- Statistics Canada. Canadian Cancer Registry (CCR) [Accessed March 9, 2020]. [updated: 2020 Jan 28]. Available at: https://www23.statcan.gc.ca/imdb/p2SV.pl?Function=getSurvey&SDDS=3207.
LinkOut - more resources
Full Text Sources
