

Transformed lymphoma: what should I do now?
- PMID: 33275671
- PMCID: PMC7727564
- DOI: 10.1182/hematology.2020000115
Transformed lymphoma: what should I do now?
Abstract
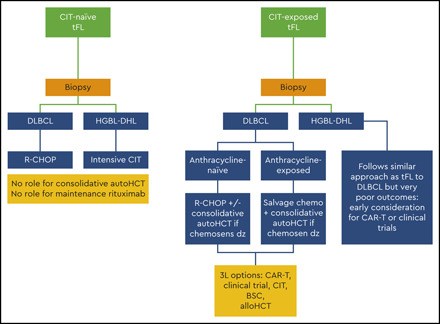
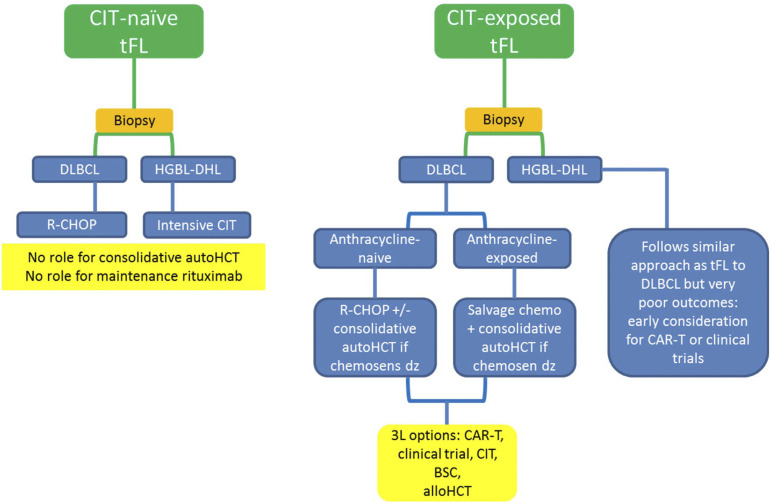
Although the majority of indolent lymphomas (focusing on follicular lymphoma [FL]) have a prolonged waxing and waning course, a portion of patients experience histologic transformation (HT) to either diffuse large B-cell lymphoma or a higher-grade morphology, often with acquisition of MYC and BCL2 and/or BCL6 rearrangements (high-grade B-cell lymphoma-double-hit lymphoma/triple-hit lymphoma). The overall incidence of HT and transformed follicular lymphoma (tFL) may be declining, but outcomes remain inferior to those in simple indolent lymphoma progression. Recent data suggest that the majority of HT cases occur in higher-risk patients with FL, and they occur early after initial chemoimmunotherapy, comprising the majority of patients with progression of disease within 24 months. This latter point emphasizes the need for a sufficient biopsy at relapse in FL. Treatment options depend on the prior therapy for the indolent component as well as the histology at relapse, but they generally follow several principles discussed in this article. Anthracycline-naïve patients have the best outcomes if there is HT, and responses to R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, prednisone) are similar to those of patients with de novo diffuse large B-cell lymphoma. Patients with anthracycline exposure prior to transformation have the best outcomes with salvage chemotherapy and a consolidative autologous stem cell transplant. However, a major challenge is the management of patients with tFL who experience relapse early after bendamustine-based treatment, in whom the role of consolidative transplant after anthracycline-based treatment is unclear. In the past several years, cellular therapy has emerged as an important tool for some but not all patients with tFL. This review focuses on the nuances of managing tFL.
© 2020 by The American Society of Hematology.
Conflict of interest statement
Conflict-of-interest disclosure: The author has served as a consultant for Janssen, Bristol-Myers Squibb, Karyopharm, Genentech, TG Therapeutics, Celgene, Bayer, and Kite in the past 2 years. There is institutional funding for clinical trials from Epizyme, Genentech, Novartis, Celgene, Portola, Karyopharm, Acerta, Pharmacyclics, TG Therapeutics, and FortySeven.
Figures

References
-
- Link BK, Maurer MJ, Nowakowski GS, et al. . Rates and outcomes of follicular lymphoma transformation in the immunochemotherapy era: a report from the University of Iowa/Mayo Clinic Specialized Program of Research Excellence Molecular Epidemiology Resource. J Clin Oncol. 2013;31(26):3272-3278. - PMC - PubMed
-
- Sarkozy C, Trneny M, Xerri L, et al. . Risk factors and outcomes for patients with follicular lymphoma who had histologic transformation after response to first-line immunochemotherapy in the PRIMA trial [published correction appears in J Clin Oncol. 2016;34(26):3230.]. J Clin Oncol. 2016;34(22):2575-2582. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous