

Platelet transfusion refractoriness: how do I diagnose and manage?
- PMID: 33275694
- PMCID: PMC7727584
- DOI: 10.1182/hematology.2020000137
Platelet transfusion refractoriness: how do I diagnose and manage?
Abstract
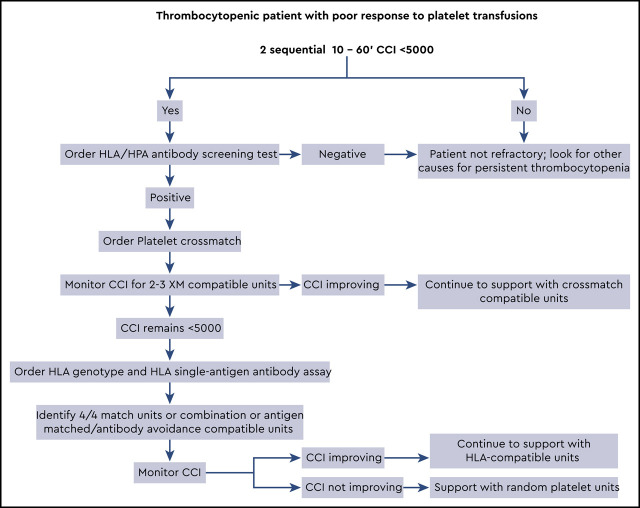
Platelet refractoriness continues to be a problem for thrombocytopenic patients because the risk of a major spontaneous or life-threatening bleed significantly increases when platelet counts drop below 10 × 109/L. The majority of patients have nonimmune causes driving the refractoriness, such as bleeding, medications, or diffuse intravascular coagulation; however, this article is dedicated to the diagnosis and support of patients with immune-based platelet refractoriness. Antibodies to class I HLA molecules (A and B alleles) are responsible for most immune-based refractory cases, with antibodies to platelet antigens seen much less frequently. Patients may be supported with either crossmatch-compatible or HLA-matched/compatible platelet units. When trying to select HLA units it can be difficult to find a perfect "4 of 4" match for the patient's class IA and IB alleles. In these cases, it is better to use the antibody specificity prediction method, which identifies compatible units that lack antigens recognized by the patient's anti-HLA antibodies. For an algorithmic approach to the patient with platelet refractoriness, see Visual Abstract.
© 2020 by The American Society of Hematology.
Conflict of interest statement
Conflict-of-interest disclosure: The author has received honoraria from Octapharma and Terumo Corporation. No other conflicts of interest to disclose.
Figures
References
-
- Forest SK, Hod EA. Management of the platelet refractory patient. Hematol Oncol Clin North Am. 2016;30(3):665-677. - PubMed
-
- Trial to Reduce Alloimmunization to Platelets Study Group. Leukocyte reduction and ultraviolet B irradiation of platelets to prevent alloimmunization and refractoriness to platelet transfusions. N Engl J Med. 1997;337(26):1861-1869. - PubMed
-
- Murphy MF, Waters AH. Platelet transfusions: the problem of refractoriness. Blood Rev. 1990;4(1):16-24. - PubMed
-
- Seftel MD, Growe GH, Petraszko T, et al. . Universal prestorage leukoreduction in Canada decreases platelet alloimmunization and refractoriness. Blood. 2004;103(1):333-339. - PubMed
-
- Bishop JF, Matthews JP, Yuen K, McGrath K, Wolf MM, Szer J. The definition of refractoriness to platelet transfusions. Transfus Med. 1992;2(1):35-41. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials