

Mortality analysis of COVID-19 infection in chronic kidney disease, haemodialysis and renal transplant patients compared with patients without kidney disease: a nationwide analysis from Turkey
- PMID: 33275763
- PMCID: PMC7716804
- DOI: 10.1093/ndt/gfaa271
Mortality analysis of COVID-19 infection in chronic kidney disease, haemodialysis and renal transplant patients compared with patients without kidney disease: a nationwide analysis from Turkey
Abstract
Background: Chronic kidney disease (CKD) and immunosuppression, such as in renal transplantation (RT), stand as one of the established potential risk factors for severe coronavirus disease 2019 (COVID-19). Case morbidity and mortality rates for any type of infection have always been much higher in CKD, haemodialysis (HD) and RT patients than in the general population. A large study comparing COVID-19 outcome in moderate to advanced CKD (Stages 3-5), HD and RT patients with a control group of patients is still lacking.
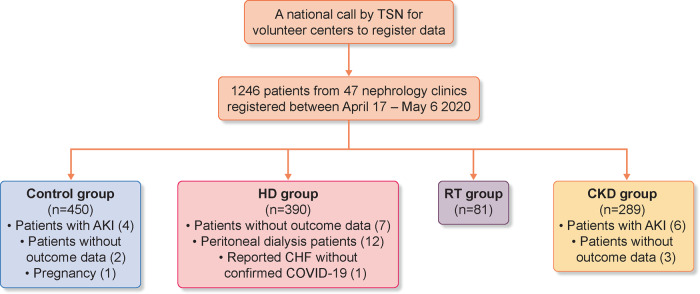
Methods: We conducted a multicentre, retrospective, observational study, involving hospitalized adult patients with COVID-19 from 47 centres in Turkey. Patients with CKD Stages 3-5, chronic HD and RT were compared with patients who had COVID-19 but no kidney disease. Demographics, comorbidities, medications, laboratory tests, COVID-19 treatments and outcome [in-hospital mortality and combined in-hospital outcome mortality or admission to the intensive care unit (ICU)] were compared.
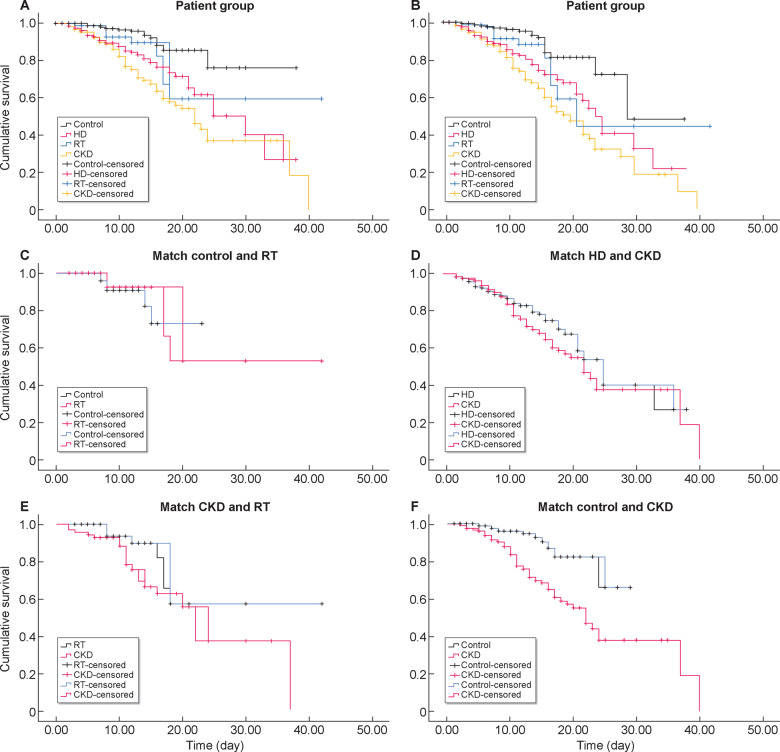
Results: A total of 1210 patients were included [median age, 61 (quartile 1-quartile 3 48-71) years, female 551 (45.5%)] composed of four groups: control (n = 450), HD (n = 390), RT (n = 81) and CKD (n = 289). The ICU admission rate was 266/1210 (22.0%). A total of 172/1210 (14.2%) patients died. The ICU admission and in-hospital mortality rates in the CKD group [114/289 (39.4%); 95% confidence interval (CI) 33.9-45.2; and 82/289 (28.4%); 95% CI 23.9-34.5)] were significantly higher than the other groups: HD = 99/390 (25.4%; 95% CI 21.3-29.9; P < 0.001) and 63/390 (16.2%; 95% CI 13.0-20.4; P < 0.001); RT = 17/81 (21.0%; 95% CI 13.2-30.8; P = 0.002) and 9/81 (11.1%; 95% CI 5.7-19.5; P = 0.001); and control = 36/450 (8.0%; 95% CI 5.8-10.8; P < 0.001) and 18/450 (4%; 95% CI 2.5-6.2; P < 0.001). Adjusted mortality and adjusted combined outcomes in CKD group and HD groups were significantly higher than the control group [hazard ratio (HR) (95% CI) CKD: 2.88 (1.52-5.44); P = 0.001; 2.44 (1.35-4.40); P = 0.003; HD: 2.32 (1.21-4.46); P = 0.011; 2.25 (1.23-4.12); P = 0.008), respectively], but these were not significantly different in the RT from in the control group [HR (95% CI) 1.89 (0.76-4.72); P = 0.169; 1.87 (0.81-4.28); P = 0.138, respectively].
Conclusions: Hospitalized COVID-19 patients with CKDs, including Stages 3-5 CKD, HD and RT, have significantly higher mortality than patients without kidney disease. Stages 3-5 CKD patients have an in-hospital mortality rate as much as HD patients, which may be in part because of similar age and comorbidity burden. We were unable to assess if RT patients were or were not at increased risk for in-hospital mortality because of the relatively small sample size of the RT patients in this study.
Keywords: COVID-19; haemodialysis; kidney disease; mortality; renal transplantation.
© The Author(s) 2020. Published by Oxford University Press on behalf of ERA-EDTA.
Figures
References
-
- Guidance to COVID-19 (SARS Cov2 Infection) (Scientific Board Study) Republic of Turkey Ministry of Health (published on April 14). https://hsgm.saglik.gov.tr/depo/birimler/goc_sagligi/covid19/rehber/COVI... (18 April 2020, date last accessed)
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
