

Is Extracorporeal Membrane Oxygenation the Standard Care for Acute Respiratory Distress Syndrome: A Systematic Review and Meta-Analysis
- PMID: 33277180
- PMCID: PMC8032315
- DOI: 10.1016/j.hlc.2020.10.014
Is Extracorporeal Membrane Oxygenation the Standard Care for Acute Respiratory Distress Syndrome: A Systematic Review and Meta-Analysis
Abstract
Background: Acute respiratory distress syndrome (ARDS) is a type of acute respiratory failure syndrome characterised by severe respiratory distress and stubborn hypoxaemia. Patients with ARDS have a prolonged hospital stay and high mortality rate. Over long-term follow-up, ARDS is found to be associated with a high incidence of long-term complications and decreased quality of life. Venovenous extracorporeal membrane oxygenation (vv-ECMO) has been widely used for the treatment of refractory ARDS. However, it is not the standard treatment as recommended by ARDS guidelines.
Aim: The aim of this study was to compare the effects of ECMO (vv-ECMO) and conventional mechanical ventilation (CMV) on the clinical outcomes in patients with ARDS.
Method: We searched the Cochrane Central Register of Controlled Trials (CENTRAL) in The Cochrane Library, Medline, EMBASE, Web of Science, and PubMed databases up to November 2019. We selected appropriate studies according to our inclusion and exclusion criteria, and extracted and analysed the data using RevMan 5.0 software to evaluate the effectiveness of ECMO systematically.
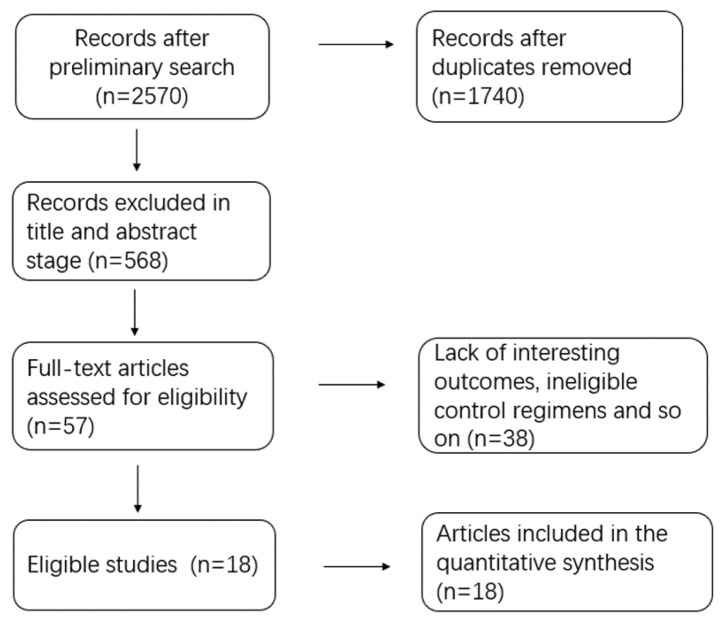
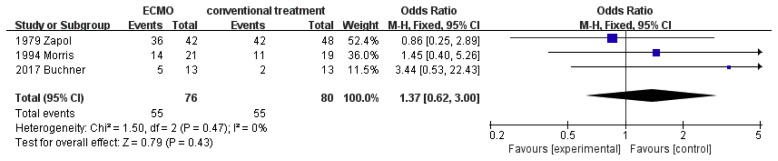
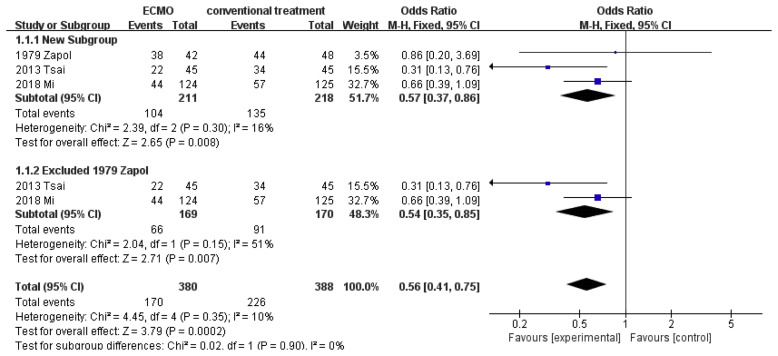
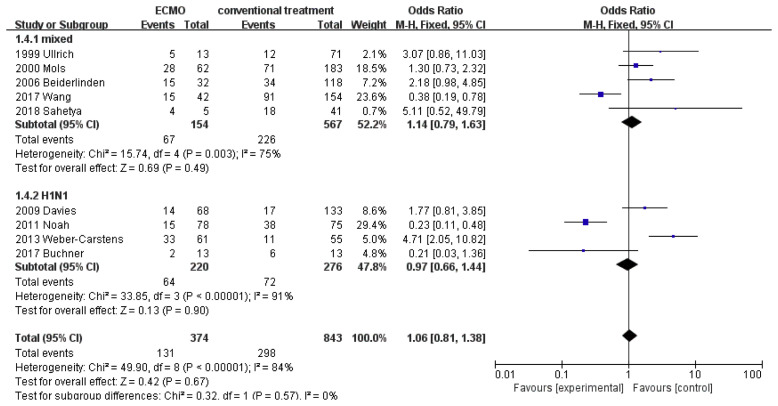
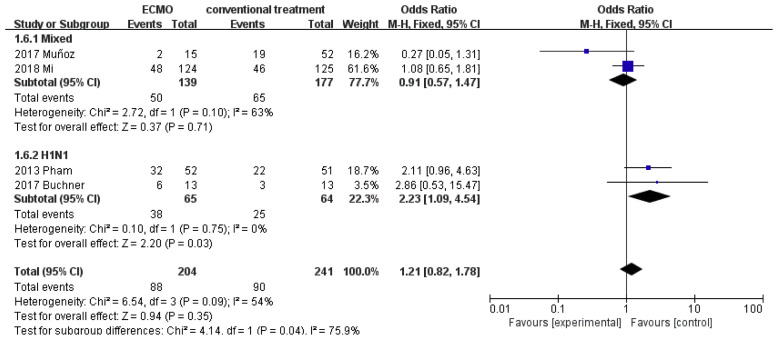
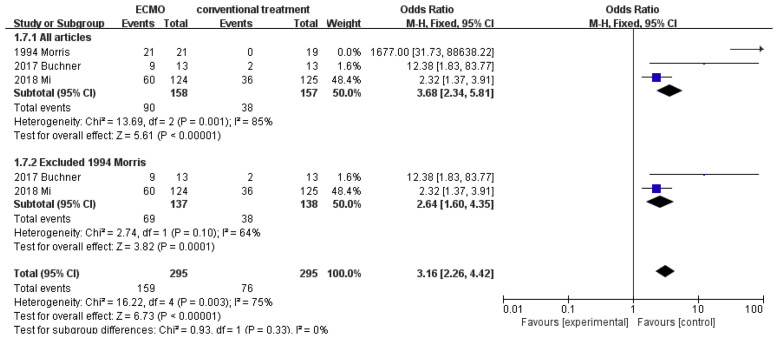
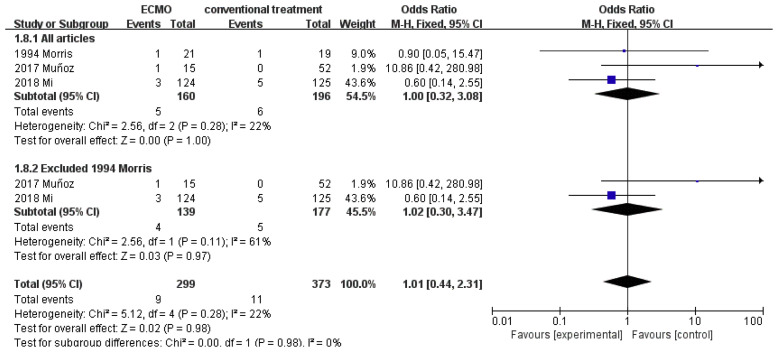
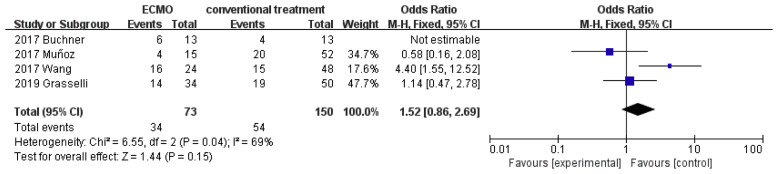
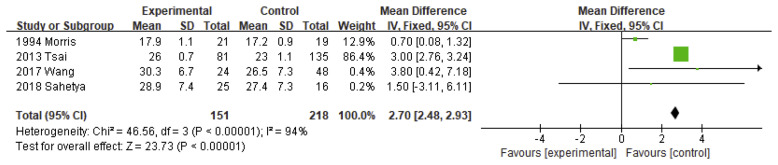
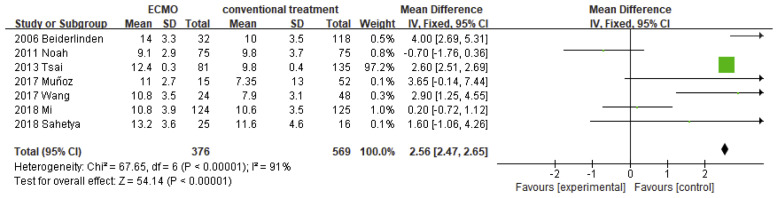
Results: A total of 18 articles and 2,399 patients were included in this meta-analysis: 898 patients in the ECMO group and 1,501 patients in the CMV group. Treatment with ECMO may be associated with reduced 1-year mortality (95% confidence interval [CI], 0.27-0.83; p=0.009) and 60-day mortality (95% CI, 0.37-0.86; p=0.008), but increased Intensive Care Unit mortality (95% CI, 1.26-2.36; p=0.0007) of patients with ARDS. Extracorporeal membrane oxygenation may not be related to 30-day mortality or complications such as nosocomial pneumonia, haemorrhagic stroke, or continuous renal replacement therapy in patients with ARDS. However, some results showed heterogeneity, such as bleeding complications and in-hospital mortality. Subgroup analysis showed that ECMO treatment might increase ICU mortality (p=0.002) and nosocomial pneumonia complications (p=0.03) in patients with H1N1 ARDS.
Conclusions: Compared with CMV, ECMO contributed to lower 60-day and 1-year mortality, and increased ICU mortality in patients with ARDS. However, H1N1 ARDS was independently associated with higher ICU mortality and nosocomial pneumonia. The results were not affected by removing retrospective control studies or articles published >20 years ago from the sensitivity analysis. This meta-analysis demonstrates the effectiveness of ECMO and its importance in standard treatment of patients with ARDS.
Keywords: ARDS; Complications; ECMO; H1N1; Mortality.
Copyright © 2020. Published by Elsevier B.V.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
