

Age-stratified discrete compartment model of the COVID-19 epidemic with application to Switzerland
- PMID: 33277545
- PMCID: PMC7718912
- DOI: 10.1038/s41598-020-77420-4
Age-stratified discrete compartment model of the COVID-19 epidemic with application to Switzerland
Abstract
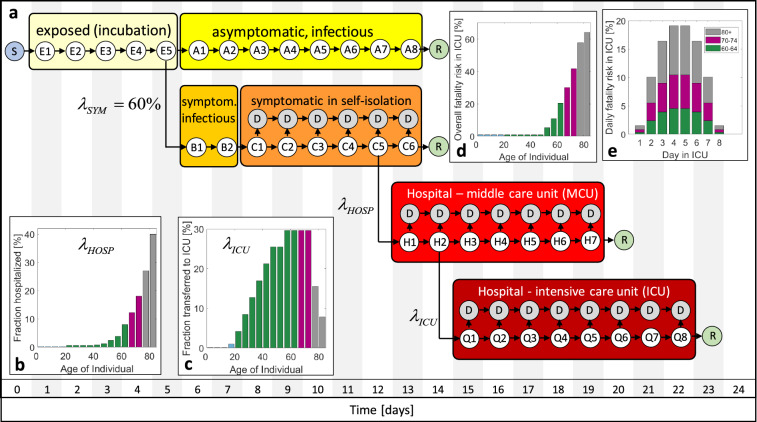
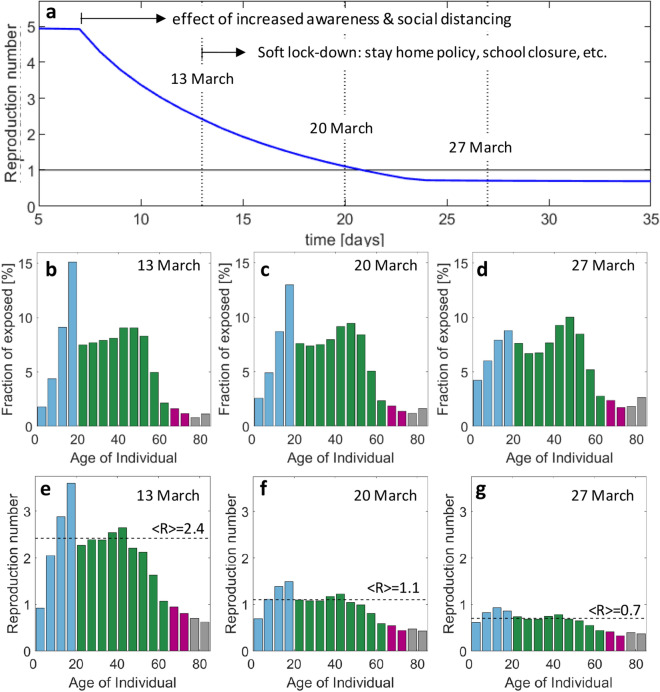
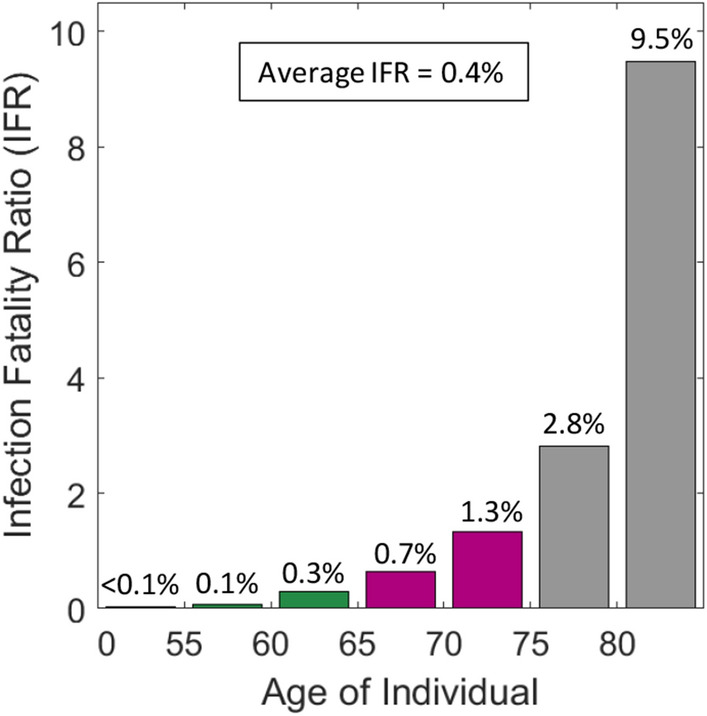
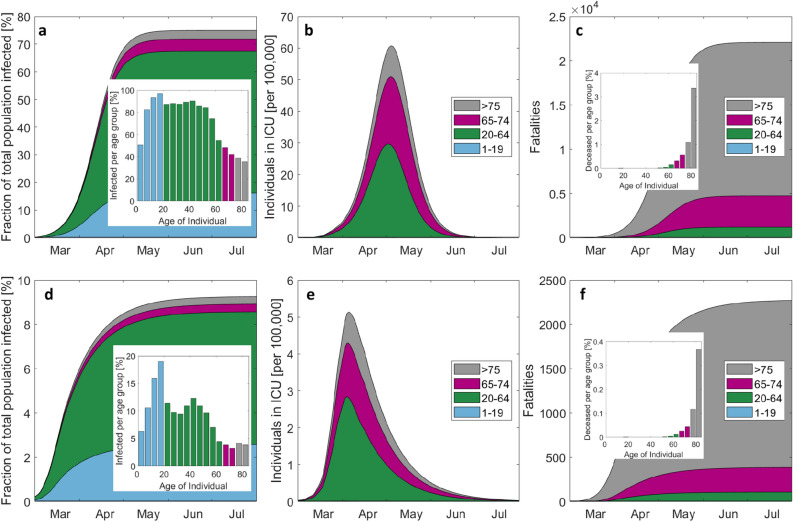
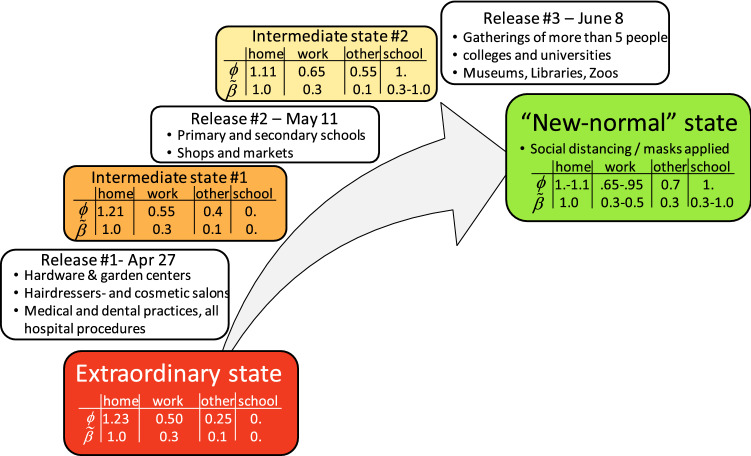
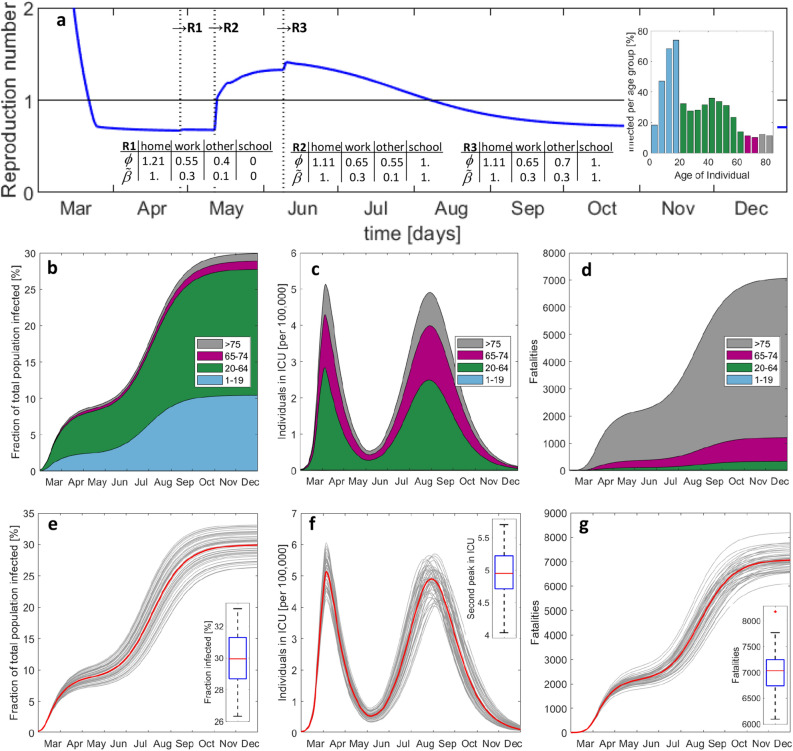
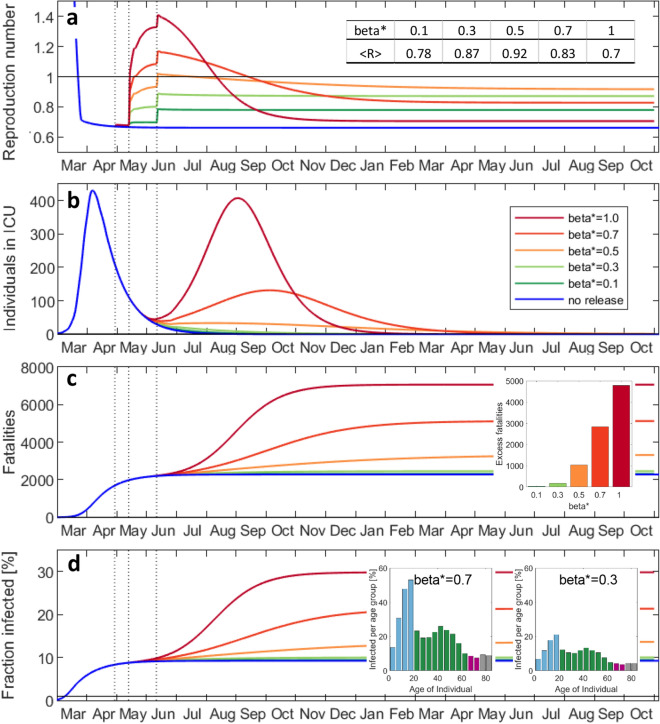
Compartmental models enable the analysis and prediction of an epidemic including the number of infected, hospitalized and deceased individuals in a population. They allow for computational case studies on non-pharmaceutical interventions thereby providing an important basis for policy makers. While research is ongoing on the transmission dynamics of the SARS-CoV-2 coronavirus, it is important to come up with epidemic models that can describe the main stages of the progression of the associated COVID-19 respiratory disease. We propose an age-stratified discrete compartment model as an alternative to differential equation based S-I-R type of models. The model captures the highly age-dependent progression of COVID-19 and is able to describe the day-by-day advancement of an infected individual in a modern health care system. The fully-identified model for Switzerland not only predicts the overall histories of the number of infected, hospitalized and deceased, but also the corresponding age-distributions. The model-based analysis of the outbreak reveals an average infection fatality ratio of 0.4% with a pronounced maximum of 9.5% for those aged ≥ 80 years. The predictions for different scenarios of relaxing the soft lockdown indicate a low risk of overloading the hospitals through a second wave of infections. However, there is a hidden risk of a significant increase in the total fatalities (by up to 200%) in case schools reopen with insufficient containment measures in place.
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Hethcote HW. The mathematics of infectious diseases. SIAM Rev. 2000 doi: 10.1137/S0036144500371907. - DOI
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
