

American College of Rheumatology Clinical Guidance for Multisystem Inflammatory Syndrome in Children Associated With SARS-CoV-2 and Hyperinflammation in Pediatric COVID-19: Version 2
- PMID: 33277976
- PMCID: PMC8559788
- DOI: 10.1002/art.41616
American College of Rheumatology Clinical Guidance for Multisystem Inflammatory Syndrome in Children Associated With SARS-CoV-2 and Hyperinflammation in Pediatric COVID-19: Version 2
Abstract
Objective: To provide guidance on the management of Multisystem Inflammatory Syndrome in Children (MIS-C), a condition characterized by fever, inflammation, and multiorgan dysfunction that manifests late in the course of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection. Recommendations are also provided for children with hyperinflammation during coronavirus disease 2019 (COVID-19), the acute, infectious phase of SARS-CoV-2 infection.
Methods: The Task Force was composed of 9 pediatric rheumatologists and 2 adult rheumatologists, 2 pediatric cardiologists, 2 pediatric infectious disease specialists, and 1 pediatric critical care physician. Preliminary statements addressing clinical questions related to MIS-C and hyperinflammation in COVID-19 were developed based on evidence reports. Consensus was built through a modified Delphi process that involved anonymous voting and webinar discussion. A 9-point scale was used to determine the appropriateness of each statement (median scores of 1-3 for inappropriate, 4-6 for uncertain, and 7-9 for appropriate). Consensus was rated as low, moderate, or high based on dispersion of the votes. Approved guidance statements were those that were classified as appropriate with moderate or high levels of consensus, which were prespecified before voting.
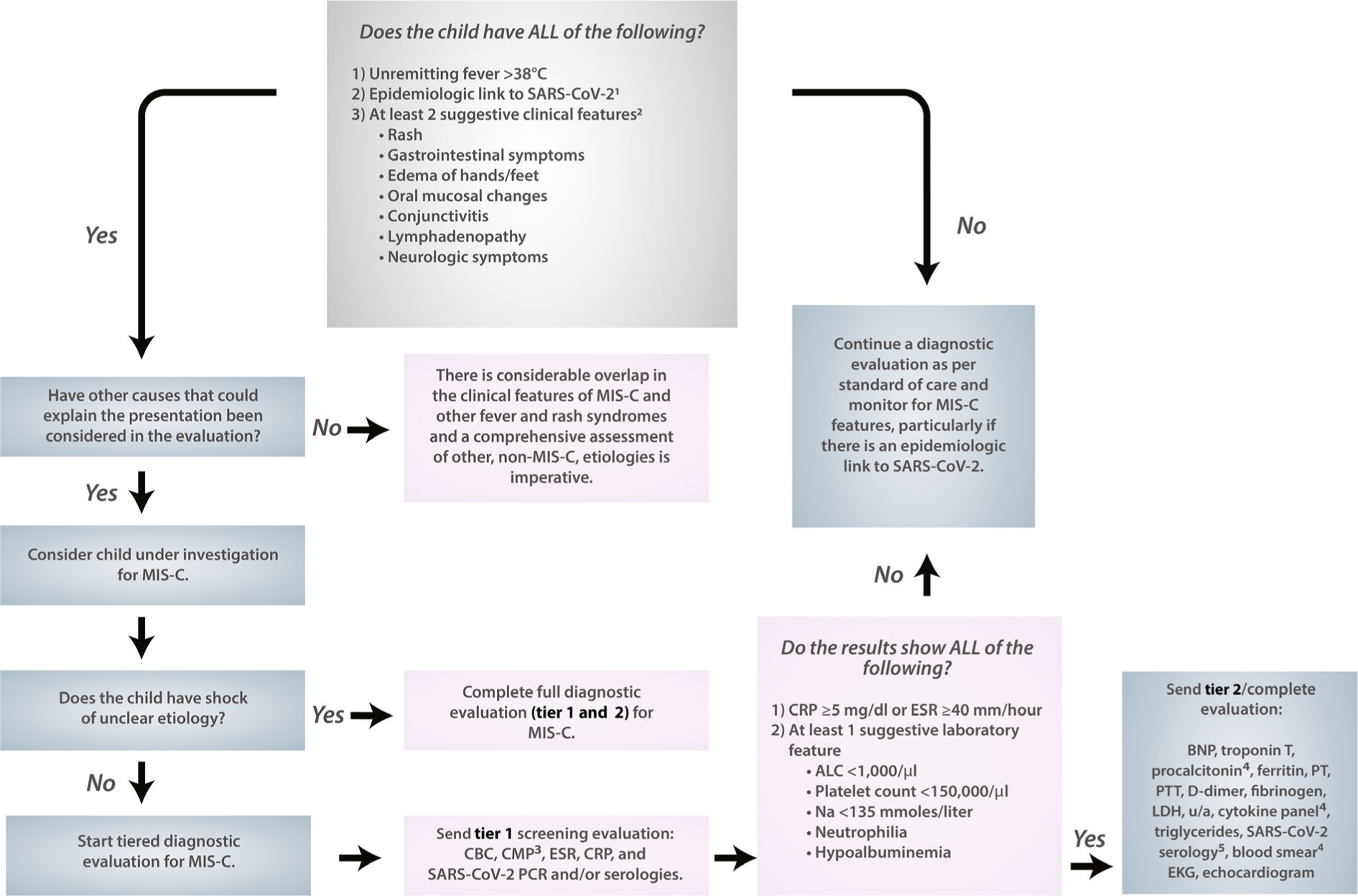
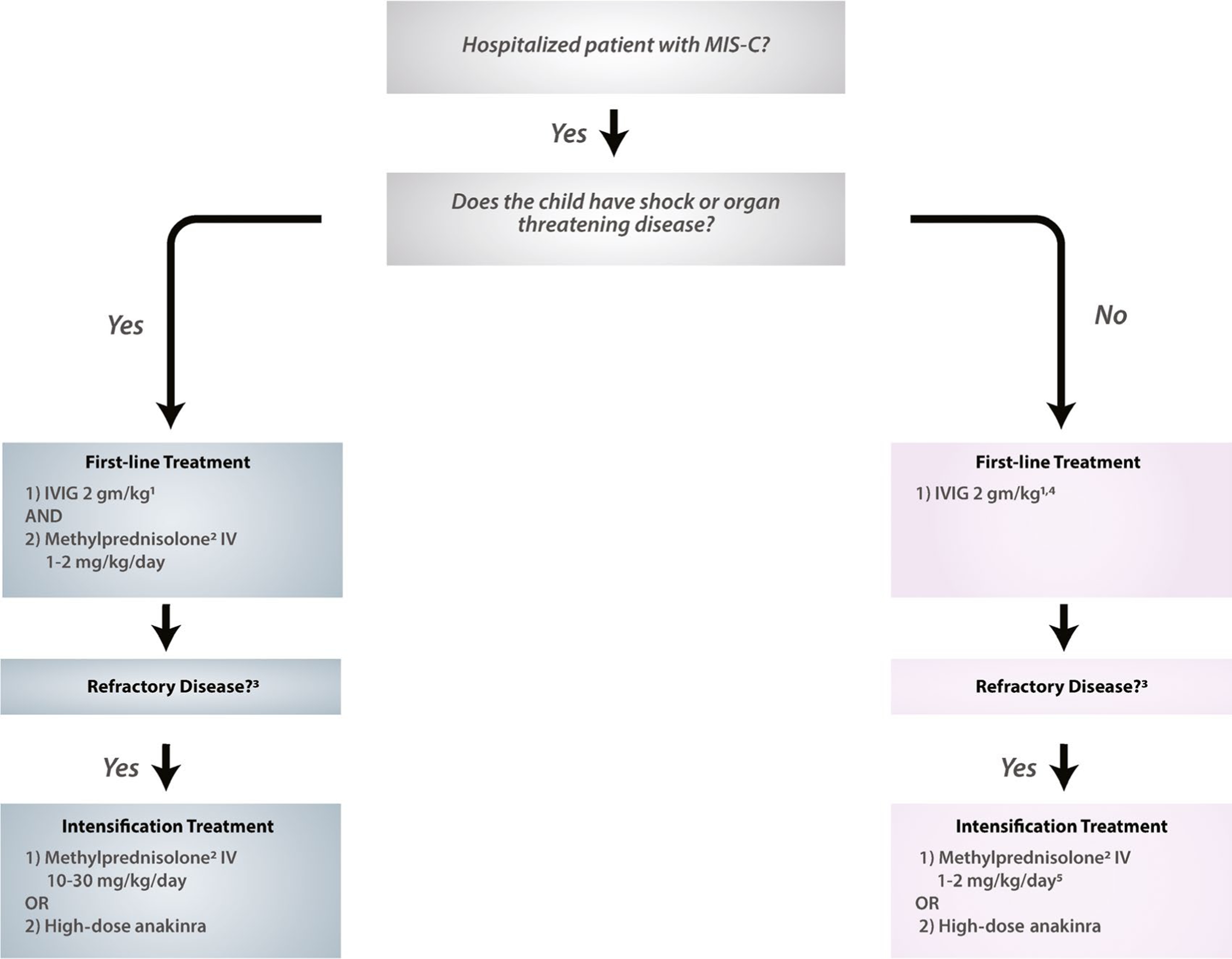
Results: The first version of the guidance was approved in June 2020, and consisted of 40 final guidance statements accompanied by a flow diagram depicting the diagnostic pathway for MIS-C. The document was revised in November 2020, and a new flow diagram with recommendations for initial immunomodulatory treatment of MIS-C was added.
Conclusion: Our understanding of SARS-CoV-2-related syndromes in the pediatric population continues to evolve. This guidance document reflects currently available evidence coupled with expert opinion, and will be revised as further evidence becomes available.
© 2020, American College of Rheumatology.
Figures
Comment in
-
Reply.Arthritis Rheumatol. 2021 Jul;73(7):1342-1343. doi: 10.1002/art.41689. Epub 2021 May 31. Arthritis Rheumatol. 2021. PMID: 33586355 No abstract available.
-
Prophylactic Anticoagulation Therapy: Comment on the Article by Henderson et al.Arthritis Rheumatol. 2021 Jul;73(7):1341-1342. doi: 10.1002/art.41690. Epub 2021 Jun 1. Arthritis Rheumatol. 2021. PMID: 33586369 No abstract available.
References
-
- World Federation of Pediatric Intensive and Critical Care Societies. Statement to the media following the 2 May Pediatric Intensive Care-COVID-19 International Collaborative conference call. May 2020. URL: http://www.wfpiccs.org/wp-content/uploads/2020/05/Media-statement-Final.pdf.
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
