

Effectiveness of seasonal malaria chemoprevention at scale in west and central Africa: an observational study
- PMID: 33278936
- PMCID: PMC7718580
- DOI: 10.1016/S0140-6736(20)32227-3
Effectiveness of seasonal malaria chemoprevention at scale in west and central Africa: an observational study
Abstract
Background: Seasonal malaria chemoprevention (SMC) aims to prevent malaria in children during the high malaria transmission season. The Achieving Catalytic Expansion of SMC in the Sahel (ACCESS-SMC) project sought to remove barriers to the scale-up of SMC in seven countries in 2015 and 2016. We evaluated the project, including coverage, effectiveness of the intervention, safety, feasibility, drug resistance, and cost-effectiveness.
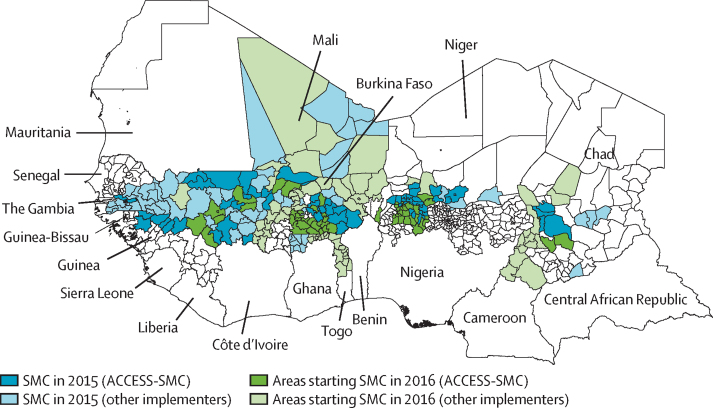
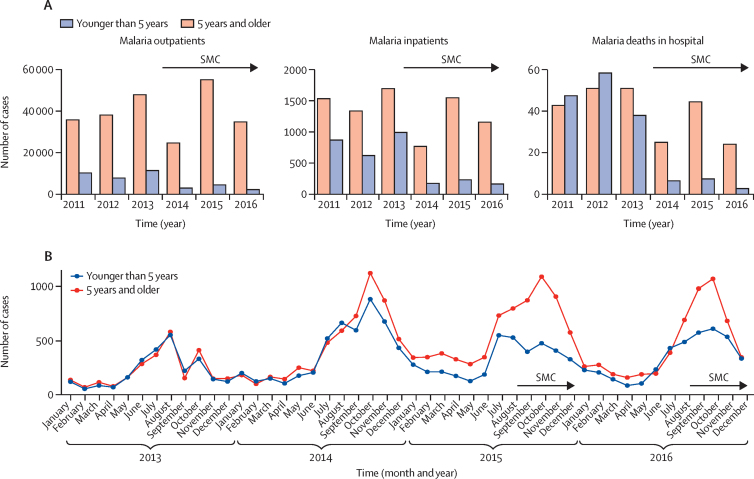
Methods: For this observational study, we collected data on the delivery, effectiveness, safety, influence on drug resistance, costs of delivery, impact on malaria incidence and mortality, and cost-effectiveness of SMC, during its administration for 4 months each year (2015 and 2016) to children younger than 5 years, in Burkina Faso, Chad, The Gambia, Guinea, Mali, Niger, and Nigeria. SMC was administered monthly by community health workers who visited door-to-door. Drug administration was monitored via tally sheets and via household cluster-sample coverage surveys. Pharmacovigilance was based on targeted spontaneous reporting and monitoring systems were strengthened. Molecular markers of resistance to sulfadoxine-pyrimethamine and amodiaquine in the general population before and 2 years after SMC introduction was assessed from community surveys. Effectiveness of monthly SMC treatments was measured in case-control studies that compared receipt of SMC between patients with confirmed malaria and neighbourhood-matched community controls eligible to receive SMC. Impact on incidence and mortality was assessed from confirmed outpatient cases, hospital admissions, and deaths associated with malaria, as reported in national health management information systems in Burkina Faso and The Gambia, and from data from selected outpatient facilities (all countries). Provider costs of SMC were estimated from financial costs, costs of health-care staff time, and volunteer opportunity costs, and cost-effectiveness ratios were calculated as the total cost of SMC in each country divided by the predicted number of cases averted.
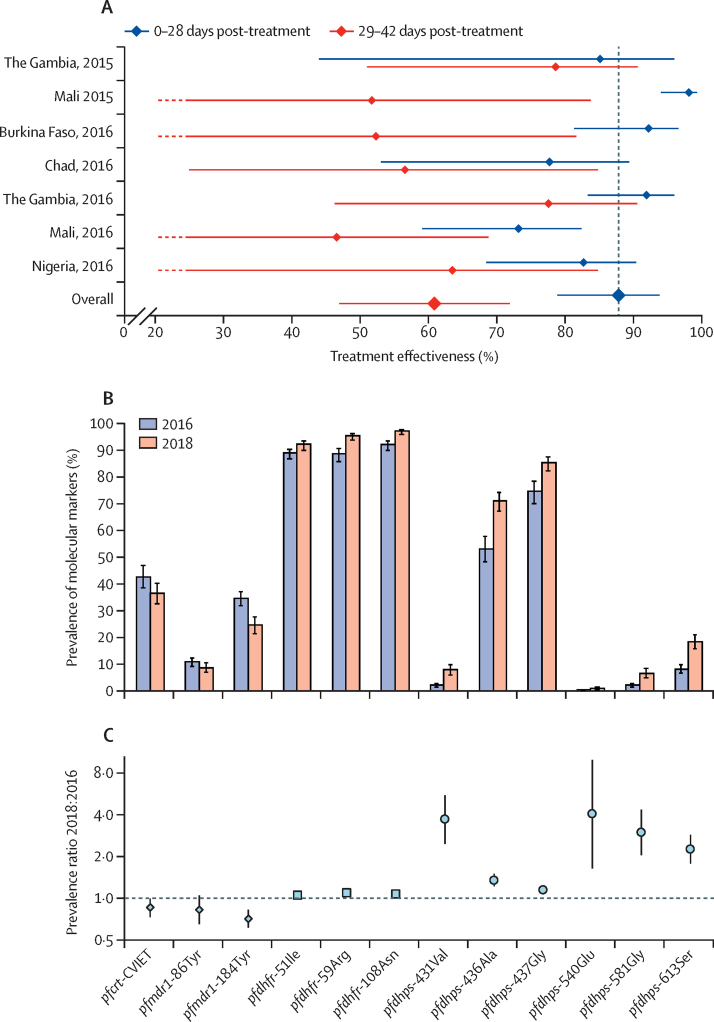
Findings: 12 467 933 monthly SMC treatments were administered in 2015 to a target population of 3 650 455 children, and 25 117 480 were administered in 2016 to a target population of 7 551 491. In 2015, among eligible children, mean coverage per month was 76·4% (95% CI 74·0-78·8), and 54·5% children (95% CI 50·4-58·7) received all four treatments. Similar coverage was achieved in 2016 (74·8% [72·2-77·3] treated per month and 53·0% [48·5-57·4] treated four times). In 779 individual case safety reports over 2015-16, 36 serious adverse drug reactions were reported (one child with rash, two with fever, 31 with gastrointestinal disorders, one with extrapyramidal syndrome, and one with Quincke's oedema). No cases of severe skin reactions (Stevens-Johnson or Lyell syndrome) were reported. SMC treatment was associated with a protective effectiveness of 88·2% (95% CI 78·7-93·4) over 28 days in case-control studies (2185 cases of confirmed malaria and 4370 controls). In Burkina Faso and The Gambia, implementation of SMC was associated with reductions in the number of malaria deaths in hospital during the high transmission period, of 42·4% (95% CI 5·9 to 64·7) in Burkina Faso and 56·6% (28·9 to 73·5) in The Gambia. Over 2015-16, the estimated reduction in confirmed malaria cases at outpatient clinics during the high transmission period in the seven countries ranged from 25·5% (95% CI 6·1 to 40·9) in Nigeria to 55·2% (42·0 to 65·3) in The Gambia. Molecular markers of resistance occurred at low frequencies. In individuals aged 10-30 years without SMC, the combined mutations associated with resistance to amodiaquine (pfcrt CVIET haplotype and pfmdr1 mutations [86Tyr and 184Tyr]) had a prevalence of 0·7% (95% CI 0·4-1·2) in 2016 and 0·4% (0·1-0·8) in 2018 (prevalence ratio 0·5 [95% CI 0·2-1·2]), and the quintuple mutation associated with resistance to sulfadoxine-pyrimethamine (triple mutation in pfdhfr and pfdhps mutations [437Gly and 540Glu]) had a prevalence of 0·2% (0·1-0·5) in 2016 and 1·0% (0·6-1·6) in 2018 (prevalence ratio 4·8 [1·7-13·7]). The weighted average economic cost of administering four monthly SMC treatments was US$3·63 per child.
Interpretation: SMC at scale was effective in preventing morbidity and mortality from malaria. Serious adverse reactions were rarely reported. Coverage varied, with some areas consistently achieving high levels via door-to-door campaigns. Markers of resistance to sulfadoxine-pyrimethamine and amodiaquine remained uncommon, but with some selection for resistance to sulfadoxine-pyrimethamine, and the situation needs to be carefully monitored. These findings should support efforts to ensure high levels of SMC coverage in west and central Africa.
Funding: Unitaid.
Copyright © 2020 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY-NC-ND 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Seasonal malaria chemoprevention: closing the know-do gap.Lancet. 2020 Dec 5;396(10265):1778-1779. doi: 10.1016/S0140-6736(20)32525-3. Lancet. 2020. PMID: 33278921 No abstract available.
References
-
- WHO . World Health Organization; Geneva: 2019. World malaria report 2018.
-
- Cissé B, Sokhna C, Boulanger D. Seasonal intermittent preventive treatment with artesunate and sulfadoxine-pyrimethamine for prevention of malaria in Senegalese children: a randomised, placebo-controlled, double-blind trial. Lancet. 2006;367:659–667. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
