

Metabolomics of exhaled breath in critically ill COVID-19 patients: A pilot study
- PMID: 33279860
- PMCID: PMC7714658
- DOI: 10.1016/j.ebiom.2020.103154
Metabolomics of exhaled breath in critically ill COVID-19 patients: A pilot study
Abstract
Background: Early diagnosis of coronavirus disease 2019 (COVID-19) is of the utmost importance but remains challenging. The objective of the current study was to characterize exhaled breath from mechanically ventilated adults with COVID-19.
Methods: In this prospective observational study, we used real-time, online, proton transfer reaction time-of-flight mass spectrometry to perform a metabolomic analysis of expired air from adults undergoing invasive mechanical ventilation in the intensive care unit due to severe COVID-19 or non-COVID-19 acute respiratory distress syndrome (ARDS).
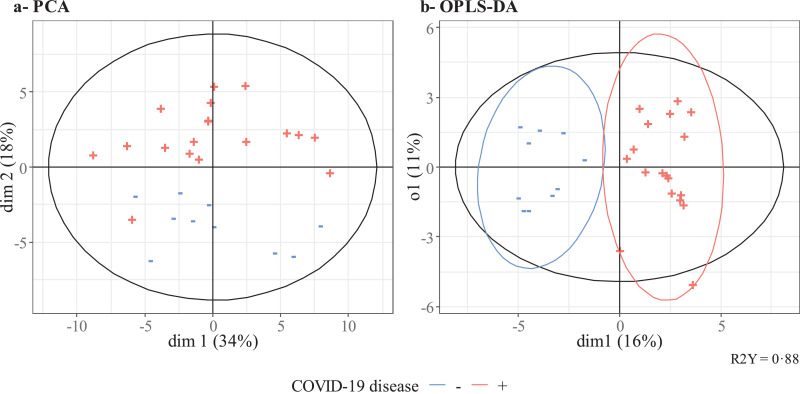
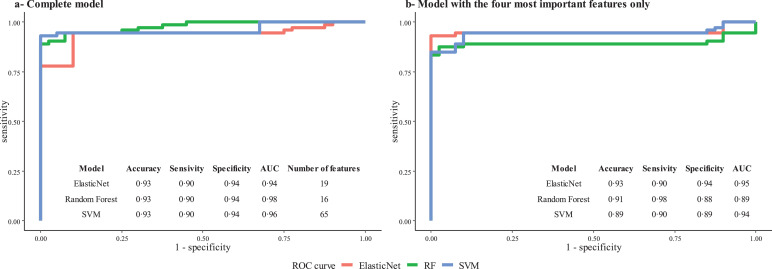
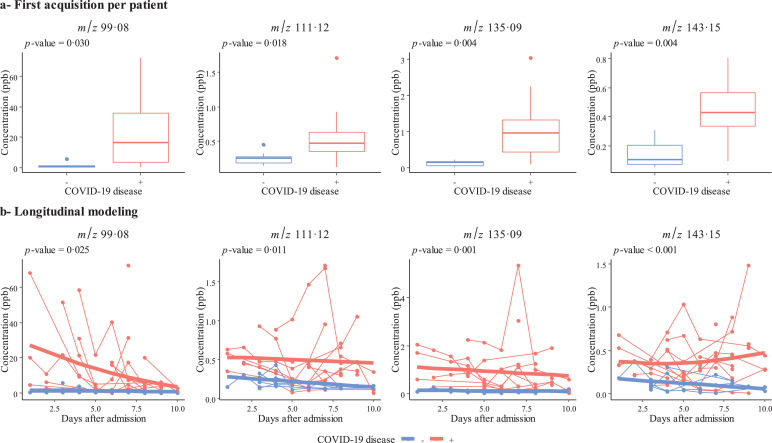
Findings: Between March 25th and June 25th, 2020, we included 40 patients with ARDS, of whom 28 had proven COVID-19. In a multivariate analysis, we identified a characteristic breathprint for COVID-19. We could differentiate between COVID-19 and non-COVID-19 ARDS with accuracy of 93% (sensitivity: 90%, specificity: 94%, area under the receiver operating characteristic curve: 0·94-0·98, after cross-validation). The four most prominent volatile compounds in COVID-19 patients were methylpent-2-enal, 2,4-octadiene 1-chloroheptane, and nonanal.
Interpretation: The real-time, non-invasive detection of methylpent-2-enal, 2,4-octadiene 1-chloroheptane, and nonanal in exhaled breath may identify ARDS patients with COVID-19.
Funding: The study was funded by Agence Nationale de la Recherche (SoftwAiR, ANR-18-CE45-0017 and RHU4 RECORDS, Programme d'Investissements d'Avenir, ANR-18-RHUS-0004), Région Île de France (SESAME 2016), and Fondation Foch.
Keywords: Breath analysis; COVID-19; Intensive care; Mechanical ventilation; Metabolomics.
Copyright © 2020 The Author(s). Published by Elsevier B.V. All rights reserved.
Figures
References
-
- COVID-19 Dashboard by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (JHU). https://coronavirus.jhu.edu/map.html (accessed October 19th, 2020).
-
- Wiersinga WJ, Rhodes A, Cheng AC, Peacock SJ, Prescott HC. Pathophysiology, transmission, diagnosis, and treatment of coronavirus disease 2019 (COVID-19): a review. JAMA. 2020;324(8):782–793. - PubMed
-
- Beigel JH, Tomashek KM, Dodd LE. Remdesivir for the treatment of COVID-19 - final report. N Engl J Med. 2020 - PubMed
-
- Recovery_Collaborative_Group. Horby P, Lim WS. Dexamethasone in hospitalized patients with COVID-19 - preliminary report. N Engl J Med. 2020
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
