

Two year outcome in nonagenarians undergoing percutaneous mitral valve repair
- PMID: 33280277
- PMCID: PMC7835616
- DOI: 10.1002/ehf2.13127
Two year outcome in nonagenarians undergoing percutaneous mitral valve repair
Abstract
Aims: Percutaneous mitral valve repair (PMVR) has emerged as standard treatment in selected patients with clinically relevant mitral regurgitation (MR) and increased surgical risk. We aimed to evaluate the safety and clinical outcomes in nonagenarians undergoing PMVR.
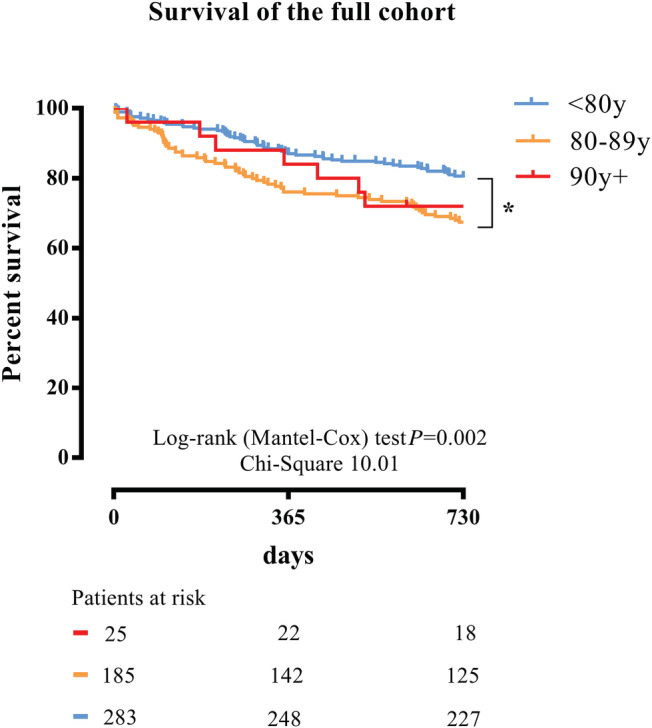
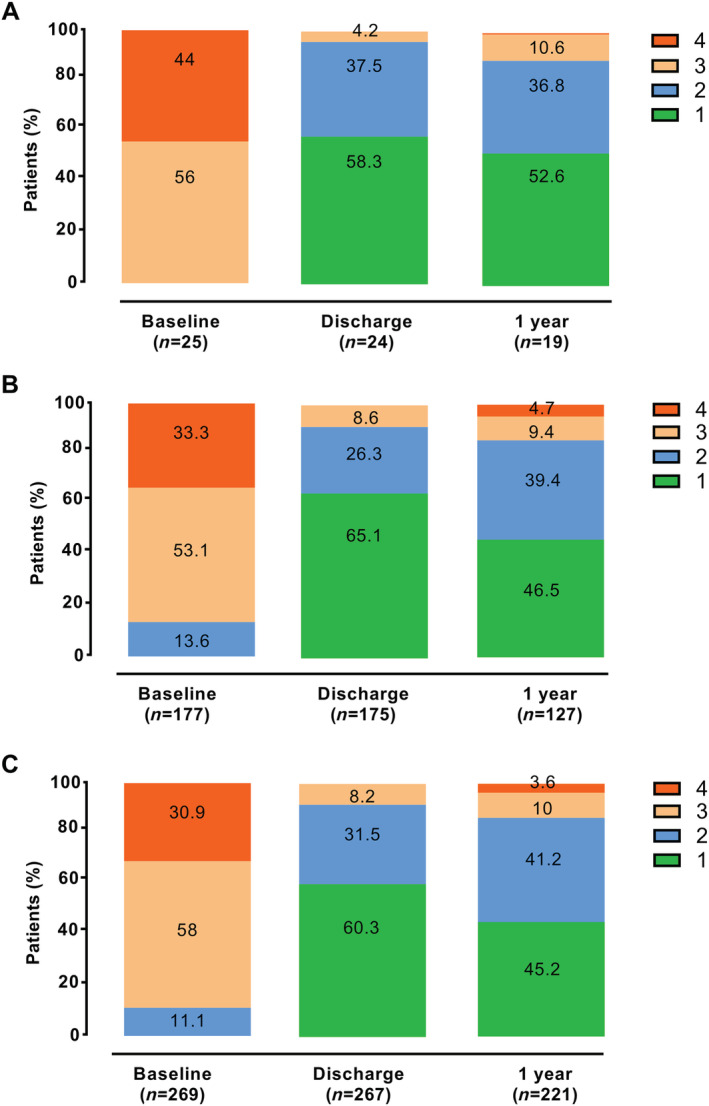
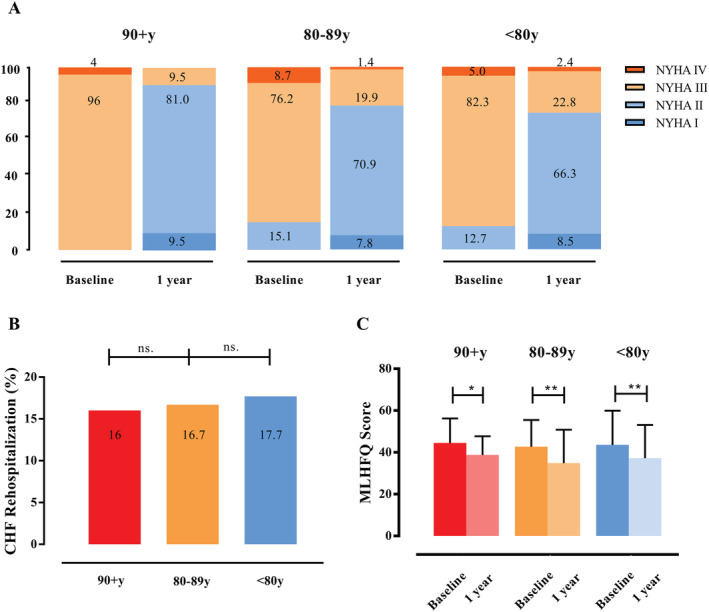
Methods and results: Altogether, 493 patients with severe MR who were treated with PMVR were included in this open-label prospective study and followed up for 2 years. We treated 25 patients with PMVR aged 90 years or above, 185 patients aged 80-89 years, and 283 patients aged <80 years. PMVR in nonagenarians was safe and did not differ from PMVR in younger patients in terms of safety endpoints. Device success did not differ among the groups (100% in nonagenarians, 95.7% in octogenarians, and 95.1% in septuagenarians, P = 0.100). Unadjusted 2 year mortality was 28% in nonagenarians, 32.4% in octogenarians, and 19.8% in septuagenarians (P = 0.008). Kaplan-Meier curves confirmed similar 2 year survival in the nonagenarian and octogenarian groups (P = 0.657). In the multivariate analysis, age [hazard ratio (HR) 1.031, 95% confidence interval (CI) 1.002-1.060, P = 0.034], higher post-procedural transmitral valve gradients (HR 1.187, 95% CI 1.104-1.277, P = 0.001), and post-procedural acute kidney injury (HR 2.360, 95% CI 1.431-3.893, P = 0.001) were independent predictors of 2 year mortality. Altogether, 89.4% of the nonagenarians, 85.9% of the octogenarians, and 86.4% of the septuagenarians had MR grade of 2+ or less at 1 year after PMVR (P = 0.910). New York Heart Association functional class improved in the vast majority of patients, irrespective of age (P = 0.129). After 1 year, 9.5% of the nonagenarians, 22.3% of the octogenarians, and 25.2% of the septuagenarians (each P = 0.001 compared with baseline) suffered from New York Heart Association Functional Class III or IV. The rate of heart failure rehospitalization in the first 12 months after PMVR did not differ among the groups (16% in the nonagenarians, 16.7% in the octogenarians, and 17.7% in the septuagenarians) (P = 0.954). Quality of life assessed by the Minnesota Living with Heart Failure Questionnaire before and at 1 year after PMVR improved in all age groups (P = 0.001).
Conclusions: Percutaneous mitral valve repair in carefully selected nonagenarians is feasible and safe with intermediate-term beneficial effects comparable with those in younger patients.
Keywords: MitraClip; Mitral regurgitation; Nonagenarians; Octogenarians; Septuagenarians.
© 2020 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
None declared.
Figures
References
-
- He W, Muenchrath MN. 90+ in the United States: 2006–2008. American Community Survey Reports (ACS–17), US Census Bureau. Washington, DC: US Government Printing Office 2011.
-
- Nkomo VT, Gardin JM, Skelton TN, Gottdiener JS, Scott CG, Enriquez‐Sarano M. Burden of valvular heart diseases: a population‐based study. Lancet 2006; 368: 1005–1011. - PubMed
-
- Baumgartner H, Falk V, Bax JJ, De Bonis M, Hamm C, Holm PJ, Iung B, Lancellotti P, Lansac E, Rodriguez Munoz D, Rosenhek R. ESC/EACTS guidelines for the management of valvular heart disease. Eur Heart J 2017; 38: 2739–2791. - PubMed
-
- Nishimura RA, Otto CM, Bonow RO, Carabello BA, Erwin JP III, Fleisher LA, Jneid H, Mack MJ, McLeod CJ, O'Gara PT, Rigolin VH. AHA/ACC focused update of the 2014 AHA/ACC guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol 2017; 70: 252–289. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
