

Exercise Reduces Ambulatory Blood Pressure in Patients With Hypertension: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
- PMID: 33280503
- PMCID: PMC7955398
- DOI: 10.1161/JAHA.120.018487
Exercise Reduces Ambulatory Blood Pressure in Patients With Hypertension: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
Abstract
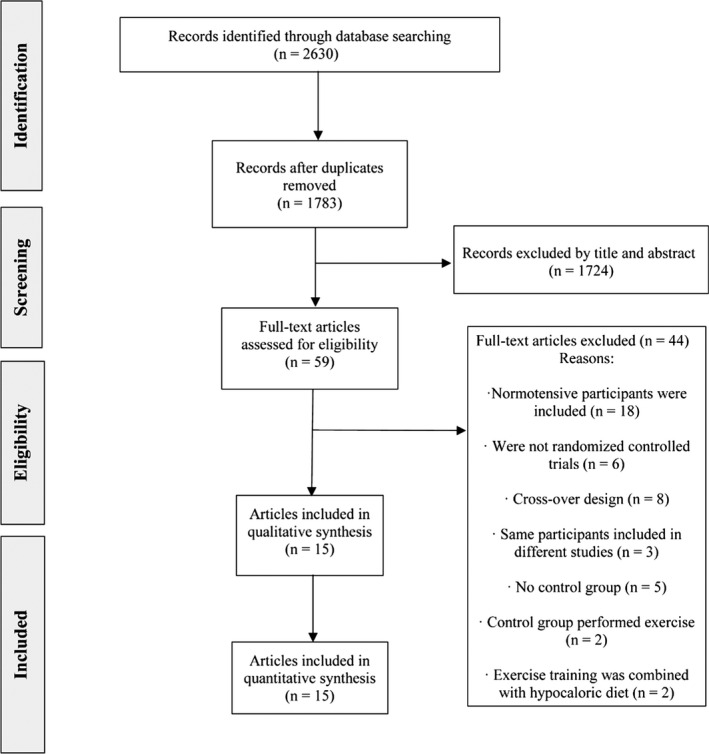
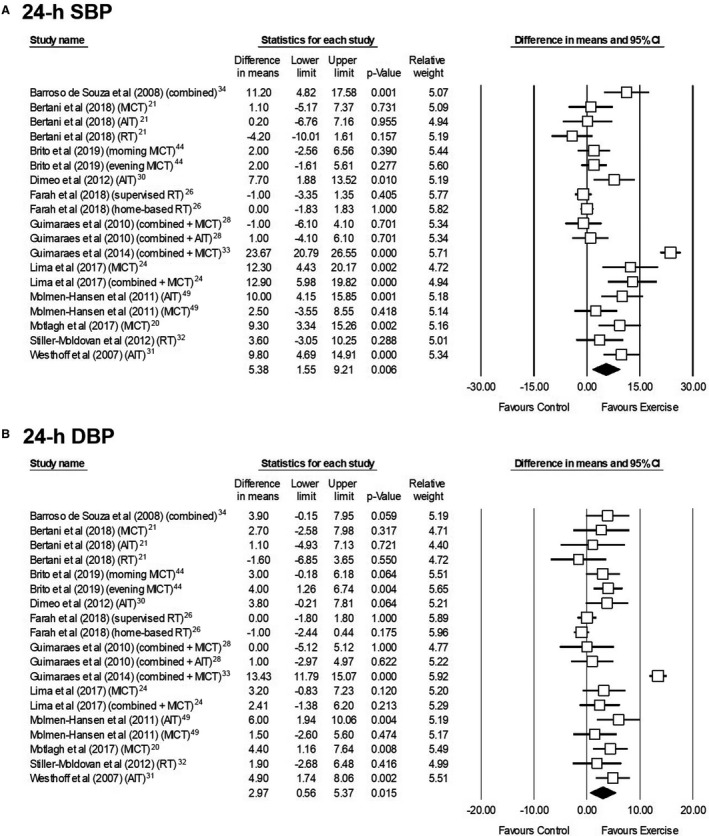
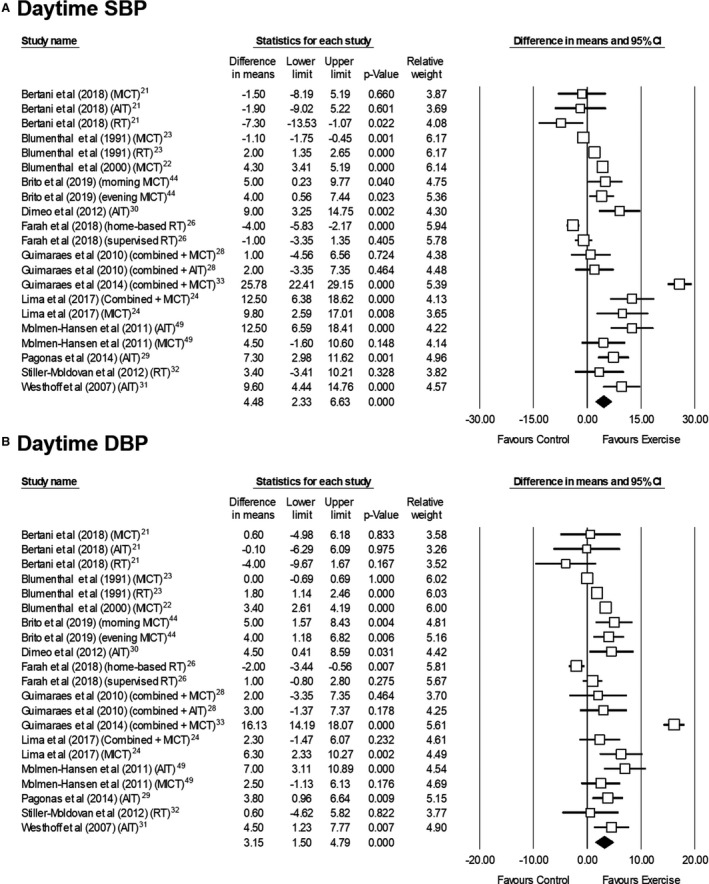
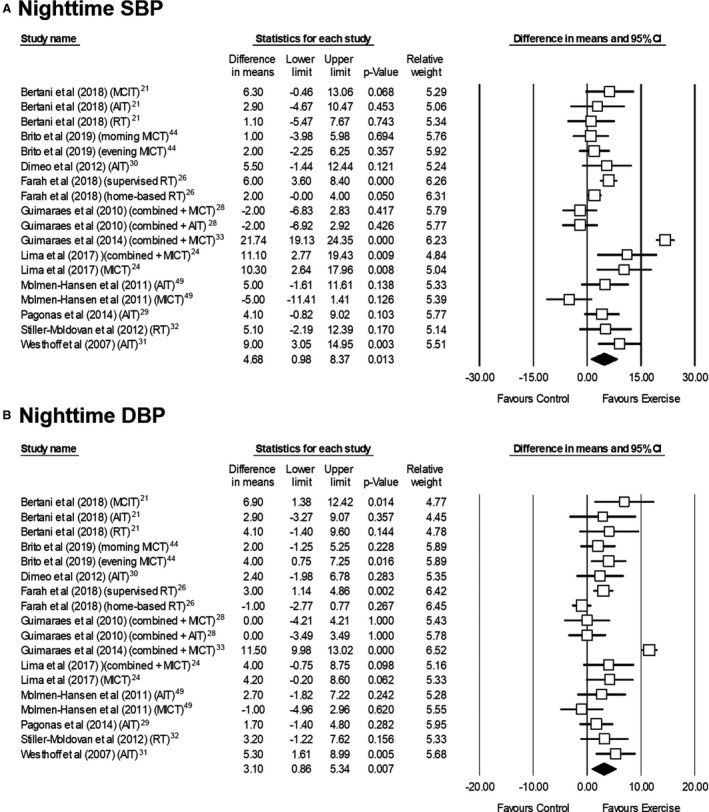
Background Although exercise training reduces office blood pressure (BP), scarcer evidence is available on whether these benefits also apply to ambulatory blood pressure (ABP), which is a stronger predictor of cardiovascular disease and mortality. The present study aims to assess the effects of exercise training on ABP in patients with hypertension based on evidence from randomized controlled trials. Methods and Results A systematic search of randomized controlled trials on the aforementioned topic was conducted in PubMed and Scopus (since inception to April 1, 2020). The mean difference between interventions (along with 95% CI) for systolic BP and diastolic BP was assessed using a random-effects model. Sub-analyses were performed attending to (1) whether participants were taking antihypertensive drugs and (2) exercise modalities. Fifteen studies (including 910 participants with hypertension) met the inclusion criteria. Interventions lasted 8 to 24 weeks (3-5 sessions/week). Exercise significantly reduced 24-hour (systolic BP, -5.4 mm Hg; [95% CI, -9.2 to -1.6]; diastolic BP, -3.0 mm Hg [-5.4 to -0.6]), daytime (systolic BP, -4.5 mm Hg [-6.6 to -2.3]; diastolic BP, -3.2 mm Hg [-4.8 to -1.5]), and nighttime ABP (systolic BP, -4.7 mm Hg [-8.4 to -1.0]; diastolic BP, -3.1 mm Hg [-5.3 to -0.9]). In separate analyses, exercise benefits on all ABP measures were significant for patients taking medication (all P<0.05) but not for untreated patients (although differences between medicated and non-medicated patients were not significant), and only aerobic exercise provided significant benefits (P<0.05). Conclusions Aerobic exercise is an effective coadjuvant treatment for reducing ABP in medicated patients with hypertension.
Keywords: blood pressure; cardiovascular risk; hypertension; physical activity.
Conflict of interest statement
None.
Figures
References
-
- Whelton PK, Carey RM, Aronow WS, Casey DE Jr, Collins KJ, Dennison Himmelfarb C, DePalma SM, Gidding S, Jamerson KA, Jones DW, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension. 2018;71:1269–1324. - PubMed
-
- Williams B, Mancia G, Spiering W, Agabiti Rosei E, Azizi M, Burnier M, Clement DL, Coca A, de Simone G, Dominiczak A, et al. 2018 ESC/ESH guidelines for the management of arterial hypertension. Eur Heart J. 2018;39:3021–3104. - PubMed
-
- Dolan E, Stanton A, Thijs L, Hinedi K, Atkins N, McClory S, Den Hond E, McCormack P, Staessen JA, O'Brien E. Superiority of ambulatory over clinic blood pressure measurement in predicting mortality: the Dublin outcome study. Hypertension. 2005;46:156–161. - PubMed
-
- Kikuya M, Ohkubo T, Asayama K, Metoki H, Obara T, Saito S, Hashimoto J, Totsune K, Hoshi H, Satoh H, et al. Ambulatory blood pressure and 10‐year risk of cardiovascular and noncardiovascular mortality: the Ohasama study. Hypertension. 2005;45:240–245. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
