

Clinical validation of three cardiovascular magnetic resonance techniques to measure strain and torsion in patients with suspected coronary artery disease
- PMID: 33280612
- PMCID: PMC7720468
- DOI: 10.1186/s12968-020-00684-2
Clinical validation of three cardiovascular magnetic resonance techniques to measure strain and torsion in patients with suspected coronary artery disease
Abstract
Background: Several cardiovascular magnetic resonance (CMR) techniques can measure myocardial strain and torsion with high accuracy. The purpose of this study was to compare displacement encoding with stimulated echoes (DENSE), tagging and feature tracking (FT) for measuring circumferential and radial myocardial strain and myocardial torsion in order to assess myocardial function and infarct scar burden both at a global and at a segmental level.
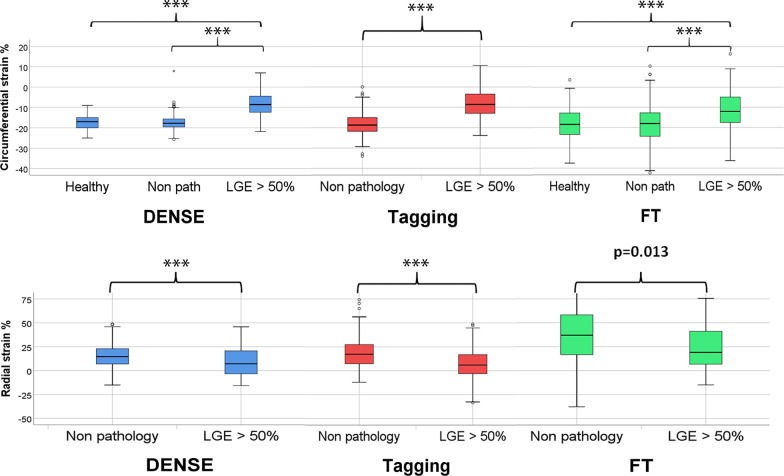
Method: 116 patients with a high likelihood of coronary artery disease (European SCORE > 15%) underwent CMR examination including cine images, tagging, DENSE and late gadolinium enhancement (LGE) in the short axis direction. In total, 97 patients had signs of myocardial disease and 19 had no abnormalities in terms of left ventricular (LV) wall mass index, LV ejection fraction, wall motion, LGE or a history of myocardial infarction. Thirty-four patients had myocardial infarct scar with a transmural LGE extent (transmurality) that exceeded 50% of the wall thickness in at least one segment. Global circumferential strain (GCS) and global radial strain (GRS) was analyzed using FT of cine loops, deformation of tag lines or DENSE displacement.
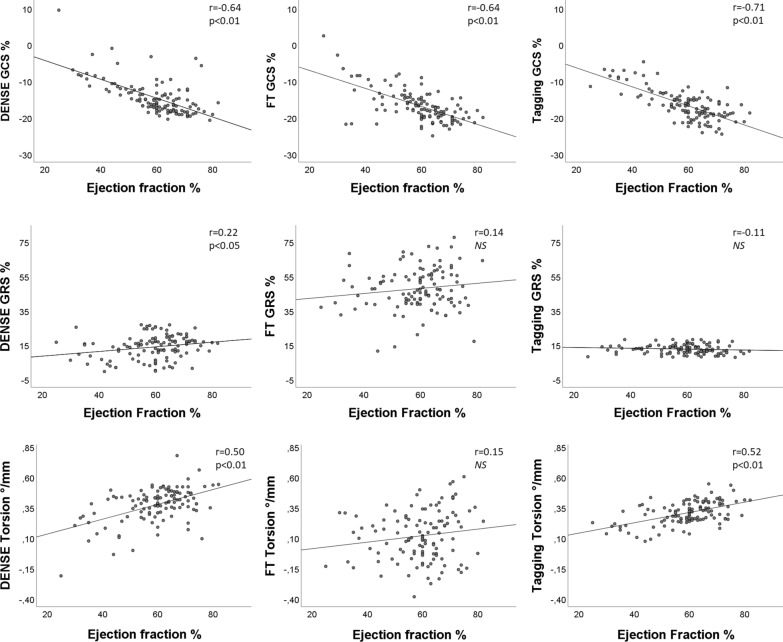
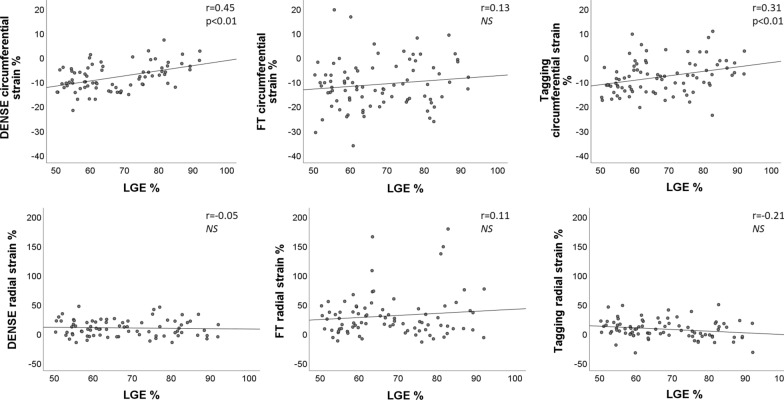
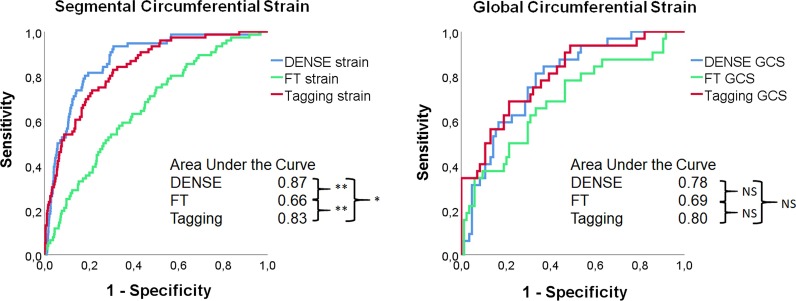
Results: DENSE and tagging both showed high sensitivity (82% and 71%) at a specificity of 80% for the detection of segments with > 50% LGE transmurality, and receiver operating characteristics (ROC) analysis showed significantly higher area under the curve-values (AUC) for DENSE (0.87) than for tagging (0.83, p < 0.001) and FT (0.66, p = 0.003). GCS correlated with global LGE when determined with DENSE (r = 0.41), tagging (r = 0.37) and FT (r = 0.15). GRS had a low but significant negative correlation with LGE; DENSE r = - 0.10, FT r = - 0.07 and tagging r = - 0.16. Torsion from DENSE and tagging had a weak correlation (- 0.20 and - 0.22 respectively) with global LGE.
Conclusion: Circumferential strain from DENSE detected segments with > 50% scar with a higher AUC than strain determined from tagging and FT at a segmental level. GCS and torsion computed from DENSE and tagging showed similar correlation with global scar size, while when computed from FT, the correlation was lower.
Keywords: DENSE; Feature tracking; Myocardial infarction; Strain; Tagging; Torsion.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
-
- Fratz S, Chung T, Greil GF, Samyn MM, Taylor AM, Valsangiacomo Buechel ER, et al. Guidelines and protocols for cardiovascular magnetic resonance in children and adults with congenital heart disease: SCMR expert consensus group on congenital heart disease. J Cardiovasc Magn Reson. 2013;15(1):1–26. doi: 10.1186/1532-429X-15-51. - DOI - PMC - PubMed
-
- Henson RE, Song SK, Pastorek JS, Ackerman JJH, Lorenz CH. Left ventricular torsion is equal in mice and humans. Am J Physiol. 2000;278(4):H1117–H1123. - PubMed
-
- Codreanu I, Robson MD, Golding SJ, Jung BA, Clarke K, Holloway CJ. Longitudinally and circumferentially directed movements of the left ventricle studied by cardiovascular magnetic resonance phase contrast velocity mapping. J Cardiovasc Magn Reson. 2010;12(1):1–8. doi: 10.1186/1532-429X-12-48. - DOI - PMC - PubMed
