

Burden of pulmonary hypertension in patients with portal hypertension in the United States: a retrospective database study
- PMID: 33282188
- PMCID: PMC7686640
- DOI: 10.1177/2045894020962917
Burden of pulmonary hypertension in patients with portal hypertension in the United States: a retrospective database study
Abstract
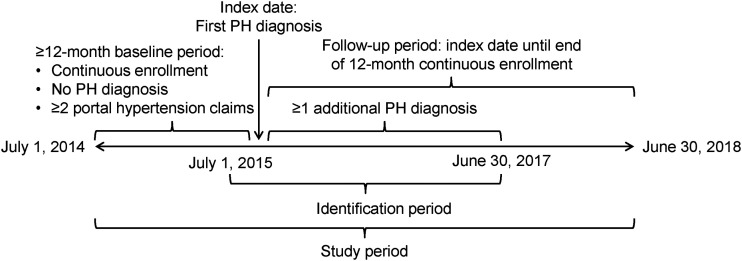
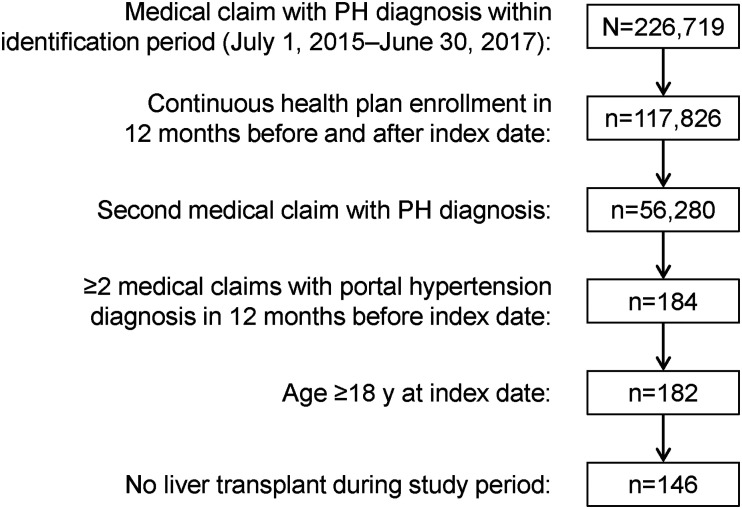
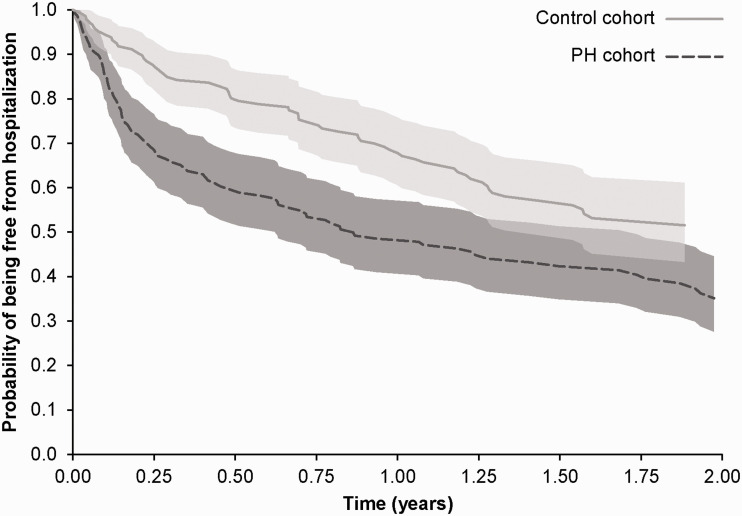
Patients with portal hypertension may develop pulmonary hypertension. The economic implications of these comorbidities have not been systematically assessed. We compared healthcare resource utilization and costs in the United States between patients with co-existing portal hypertension and pulmonary hypertension (pulmonary hypertension cohort) and a matched cohort of portal hypertension patients without pulmonary hypertension (control cohort). In this retrospective analysis, adult pulmonary hypertension and control patients were identified from the Optum® Clinformatics® Data Mart database between 1 July 2014 and 30 June 2018. All patients had ≥2 claims with diagnosis codes for portal hypertension; pulmonary hypertension patients had ≥2 claims with diagnosis codes for pulmonary hypertension; controls could not have pulmonary hypertension diagnoses or any claims for pulmonary arterial hypertension-specific medications. Controls were matched to pulmonary hypertension patients by age, sex, Charlson comorbidity index score, and liver diseases. We assessed 12-month healthcare resource utilization and costs. Each cohort included 146 patients. During follow-up, pulmonary hypertension cohort patients were more likely than controls to experience a hospitalization (51% vs. 32%, P = 0.0014) and an emergency room visit (55% vs. 41%, P = 0.026). The average annual total cost was higher in pulmonary hypertension patients than for matched controls ($119,912 vs. $81,839, P < 0.0001). After covariate adjustment, costs for pulmonary hypertension cohort patients were 1.47 times higher than those for controls (P = 0.0197). These findings suggest that patients with portal hypertension and co-existing pulmonary hypertension are at a greater risk for hospitalization and incur higher mean annual total costs than portal hypertension patients without pulmonary hypertension.
Keywords: healthcare resource utilization; hospitalization; portal hypertension; portopulmonary hypertension; pulmonary arterial hypertension.
© The Author(s) 2020.
Conflict of interest statement
Conflict of interest: The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: SS has served on advisory committees for Actelion, Bayer and United Therapeutics, and has received consultancy, steering committee, and speaker bureau fees from Actelion, Bayer and United Therapeutics; travel/accommodation reimbursement from Actelion for presenting at the International Society for Heart and Lung Transplantation meeting 2019; and grant support from the ACCP Chest PAH Research Award 2017. YT, MF, PA, and RD are employees of Actelion Pharmaceuticals US, Inc., a Janssen Pharmaceutical Company of Johnson & Johnson, and hold stock in Johnson & Johnson.
Figures
References
-
- Galiè N, Hoeper MM, Humbert M, et al. Guidelines for the diagnosis and treatment of pulmonary hypertension: the Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS), endorsed by the International Society of Heart and Lung Transplantation (ISHLT). Eur Heart J 2009; 30: 2493–2537. - PubMed
-
- Simonneau G, Gatzoulis MA, Adatia I, et al. Updated clinical classification of pulmonary hypertension. J Am Coll Cardiol 2013; 62: D34–D41. - PubMed
LinkOut - more resources
Full Text Sources
