

Thoracic positron emission tomography: 18F-fluorodeoxyglucose and beyond
- PMID: 33282403
- PMCID: PMC7711422
- DOI: 10.21037/jtd-2019-cptn-09
Thoracic positron emission tomography: 18F-fluorodeoxyglucose and beyond
Abstract
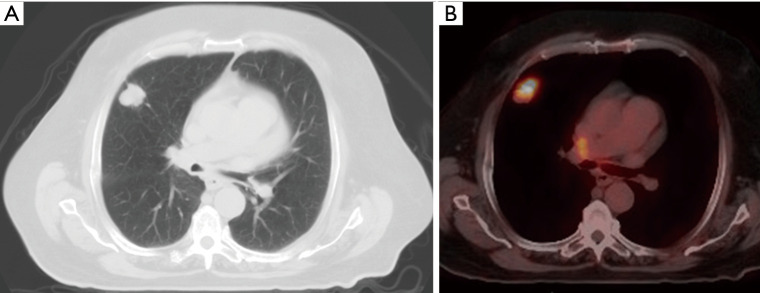
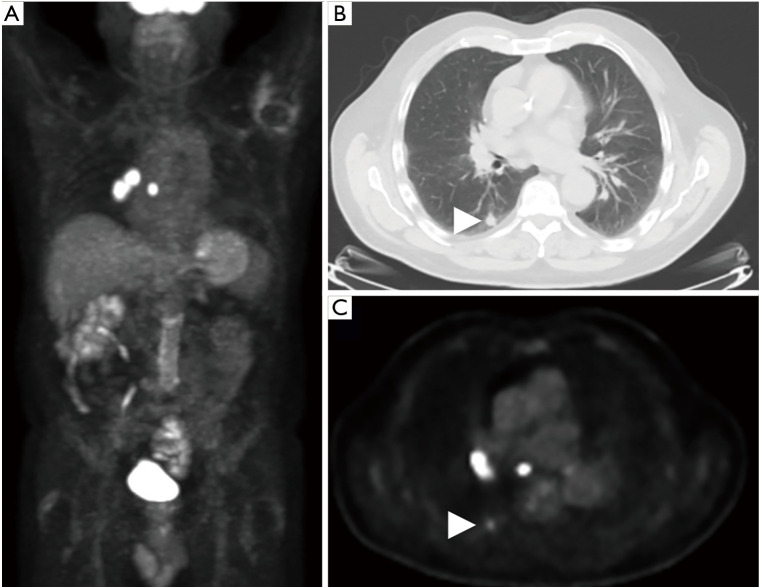
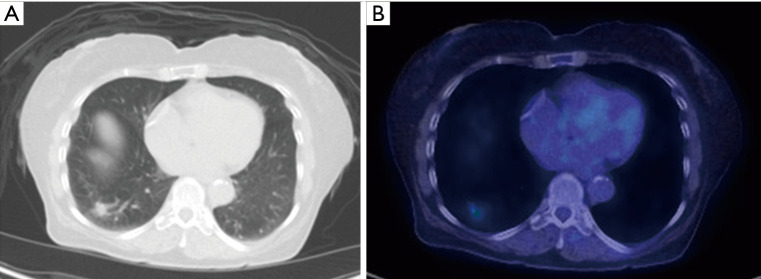
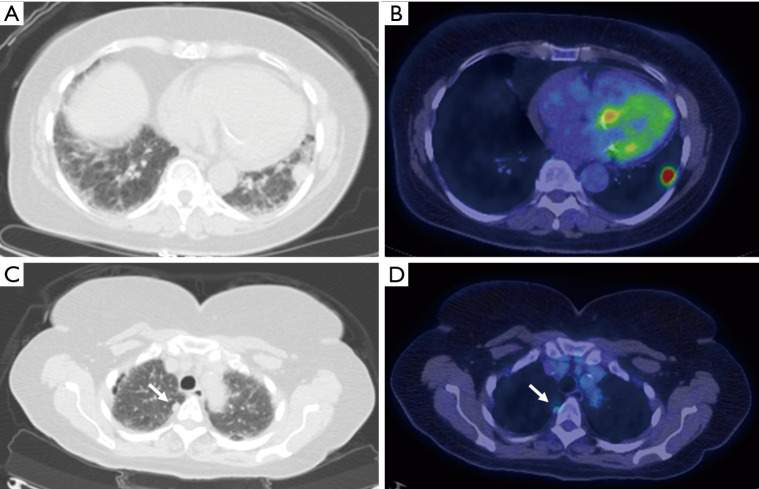
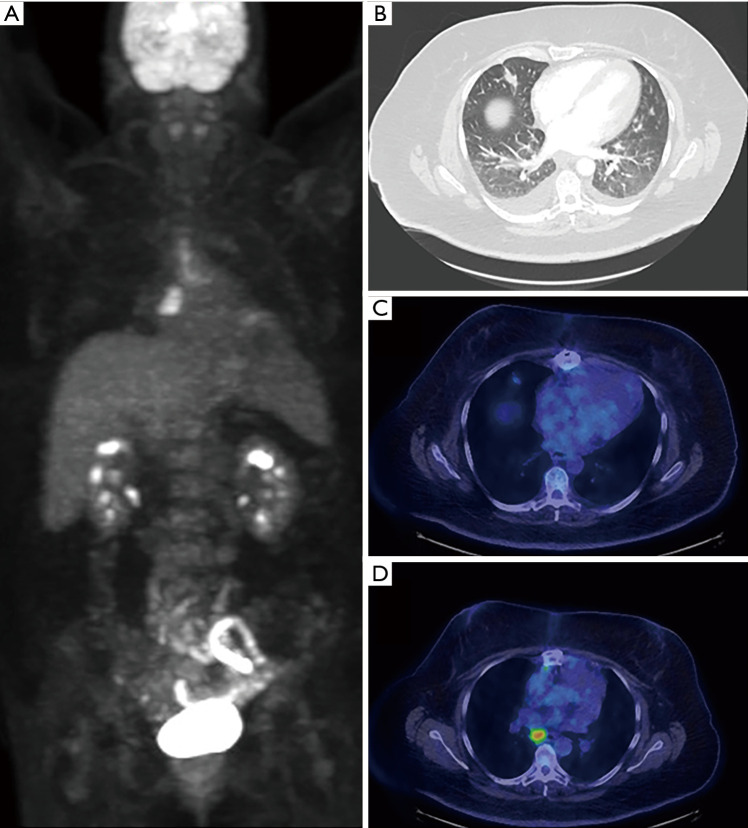
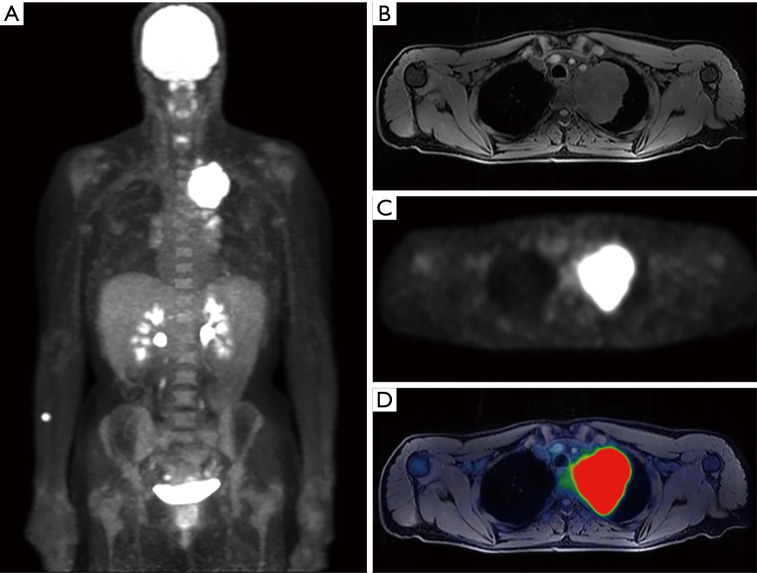
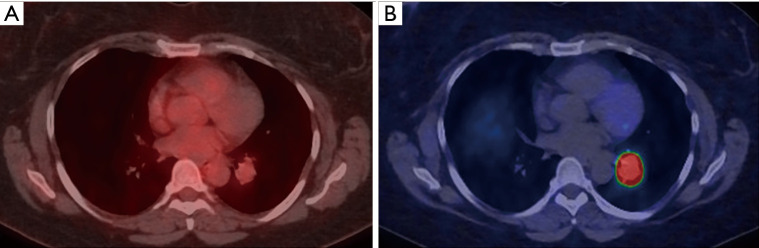
Ongoing technologic and therapeutic advancements in medicine are now testing the limits of conventional anatomic imaging techniques. The ability to image physiology, rather than simply anatomy, is critical in the management of multiple disease processes, especially in oncology. Nuclear medicine has assumed a leading role in detecting, diagnosing, staging and assessing treatment response of various pathologic entities, and appears well positioned to do so into the future. When combined with computed tomography (CT) or magnetic resonance imaging (MRI), positron emission tomography (PET) has become the sine quo non technique of evaluating most solid tumors especially in the thorax. PET/CT serves as a key imaging modality in the initial evaluation of pulmonary nodules, often obviating the need for more invasive testing. PET/CT is essential to staging and restaging in bronchogenic carcinoma and offers key physiologic information with regard to treatment response. A more recent development, PET/MRI, shows promise in several specific lung cancer applications as well. Additional recent advancements in the field have allowed PET to expand beyond imaging with 18F-flurodeoxyglucose (FDG) alone, now with the ability to specifically image certain types of cell surface receptors. In the thorax this predominantly includes 68Ga-DOTATATE which targets the somatostatin receptors abundantly expressed in neuroendocrine tumors, including bronchial carcinoid. This receptor targeted imaging technique permits targeting these tumors with therapeutic analogues such as 177Lu labeled DOTATATE. Overall, the proper utilization of PET in the thorax has the ability to directly impact and improve patient care.
Keywords: Positron emission tomography (PET); bronchogenic carcinoma; positron emission tomography/computed tomography (PET/CT); positron emission tomography/magnetic resonance imaging (PET/MRI); pulmonary nodule.
2020 Journal of Thoracic Disease. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at: http://dx.doi.org/10.21037/jtd-2019-cptn-09). The series “Contemporary Practice in Thoracic Neoplasm Diagnosis, Evaluation and Treatment” was commissioned by the editorial office without any funding or sponsorship. The authors have no other conflicts of interest to declare.
Figures




References
-
- Bunyaviroch T, Coleman RE. PET evaluation of lung cancer. J Nucl Med 2006;47:451-69. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous