

Discordant Echocardiographic Grading in Low Gradient Aortic Stenosis (DEGAS Study) From the Italian Society of Echocardiography and Cardiovascular Imaging Research Network: Rationale and Study Design
- PMID: 33282641
- PMCID: PMC7706377
- DOI: 10.4103/jcecho.jcecho_68_20
Discordant Echocardiographic Grading in Low Gradient Aortic Stenosis (DEGAS Study) From the Italian Society of Echocardiography and Cardiovascular Imaging Research Network: Rationale and Study Design
Abstract
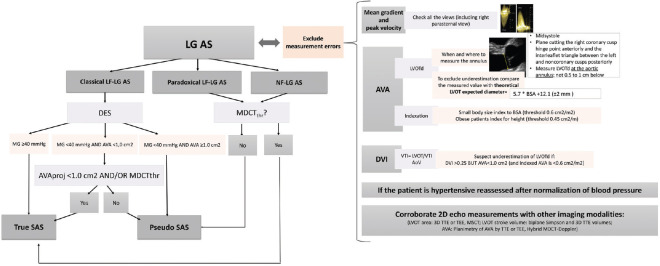
Background: Low-gradient aortic stenosis (LG-AS) is characterized by the combination of an aortic valve area compatible with severe stenosis and a low transvalvular mean gradient with low-flow state (i.e., indexed stroke volume <35 mL/m2) in the presence of reduced (classical low-flow AS) or preserved (paradoxical low-flow AS) ejection fraction. Furthermore, the occurrence of a normal-flow LG-AS is still advocated by many authors. Within this diagnostic complexity, the diagnosis of severe AS remains challenging.
Objective: The general objective of the Discordant Echocardiographic Grading in Low-gradient AS (DEGAS Study) study will be to assess the prevalence of true severe AS in this population and validate new parameters to improve the assessment and the clinical decision-making in patients with LG-AS.
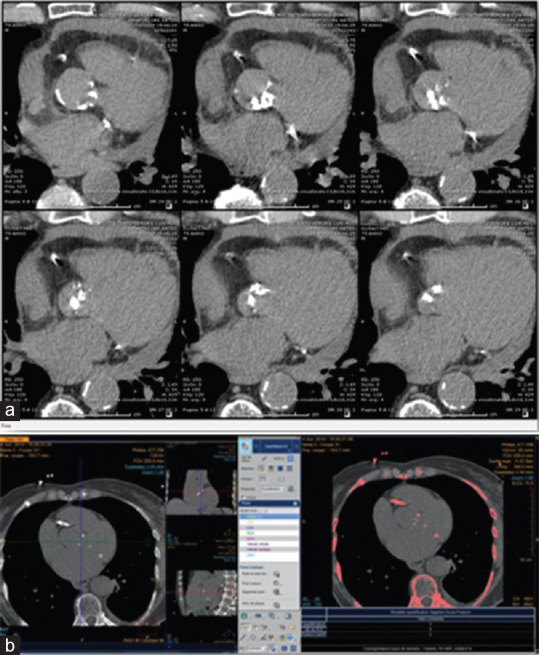
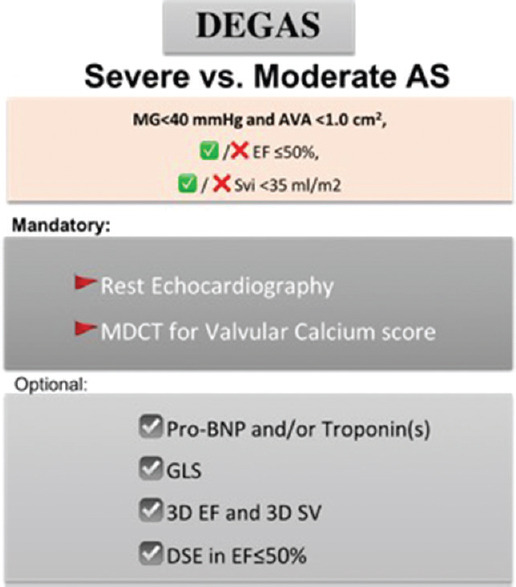
Methods and analyses: The DEGAS Study of the Italian Society of Echocardiography and Cardiovascular Imaging is a prospective, multicenter, observational diagnostic study that will enroll consecutively adult patients with LG-AS over 2 years. AS severity will be ideally confirmed by a multimodality approach, but only the quantification of calcium score by multidetector computed tomography will be mandatory. The primary clinical outcome variable will be 12-month all-cause mortality. The secondary outcome variables will be (i) 30-day mortality (for patients treated by Surgical aortic valve replacement or TAVR); (ii) 12-month cardiovascular mortality; (iii) 12-month new major cardiovascular events such as myocardial infarction, stroke, vascular complications, and rehospitalization for heart failure; and (iv) composite endpoint of cardiovascular mortality and hospitalization for heart failure. Data collection will take place through a web platform (REDCap), absolutely secure based on current standards concerning the ethical requirements and data integrity.
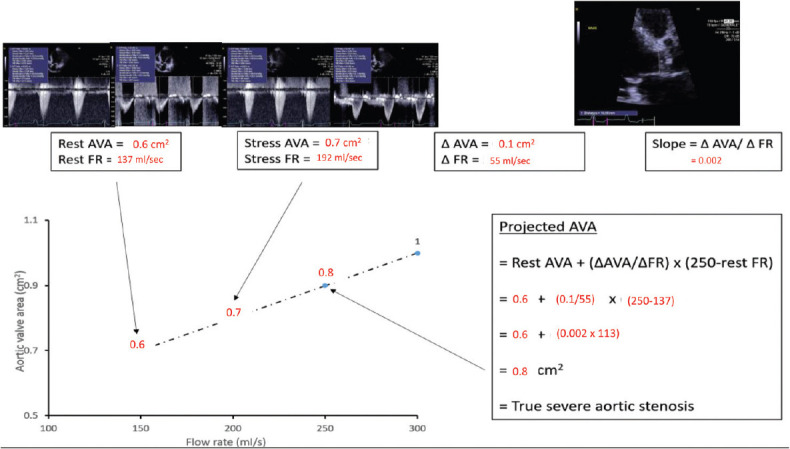
Keywords: Aortic valve calcium score; aortic valve stenosis; diagnosis; dobutamine stress echocardiography; echocardiography.
Copyright: © 2020 Journal of Cardiovascular Echography.
Conflict of interest statement
There are no conflicts of interest.
Figures
References
-
- Dulgheru R, Pibarot P, Sengupta PP, Piérard LA, Rosenhek R, Magne J, et al. Multimodality imaging strategies for the assessment of aortic stenosis: Viewpoint of the heart valve clinic international database (HAVEC) Group. Circ Cardiovasc Imaging. 2016;9:e004352. - PubMed
-
- Delgado V, Clavel MA, Hahn RT, Gillam L, Bax J, Sengupta PP, et al. How do we reconcile echocardiography, computed tomography, and hybrid imaging in assessing discordant grading of aortic stenosis severity? JACC Cardiovasc Imaging. 2019;12:267–82. - PubMed
-
- Ternacle J, Clavel MA. Assessment of Aortic Stenosis Severity: A Multimodality Approach. Cardiol Clin. 2020;38:13–22. - PubMed
-
- Guzzetti E, Pibarot P, Clavel MA. Normal-flow low-gradient severe aortic stenosis is a frequent and real entity. Eur Heart J Cardiovasc Imaging. 2019;20:1102–4. - PubMed