

Increased mortality and worse cardiac outcome of acute myocardial infarction during the early COVID-19 pandemic
- PMID: 33283476
- PMCID: PMC7835606
- DOI: 10.1002/ehf2.13075
Increased mortality and worse cardiac outcome of acute myocardial infarction during the early COVID-19 pandemic
Abstract
Aims: This study aimed to evaluate the impact of coronavirus disease 2019 (Covid-19) outbreak on admissions for acute myocardial infarction (AMI) and related mortality, severity of presentation, major cardiac complications and outcome in a tertiary-care university hospital in Berlin, Germany.
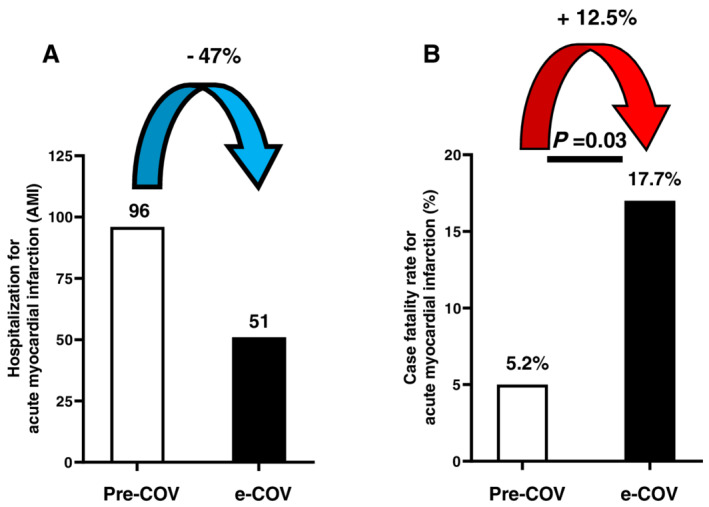
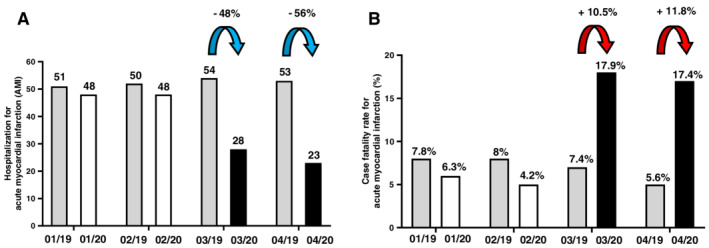
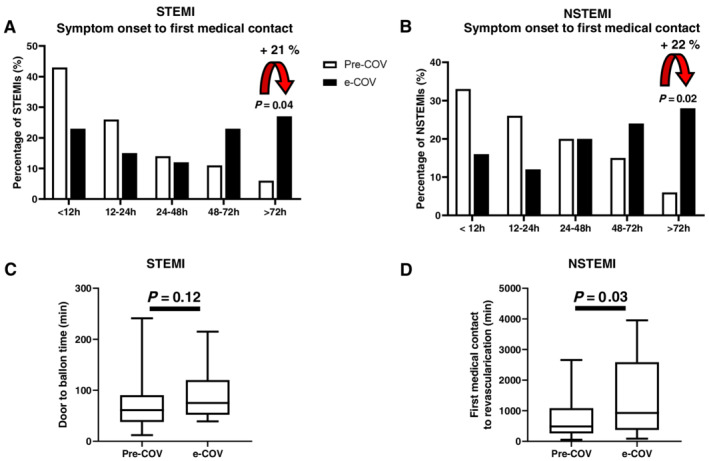
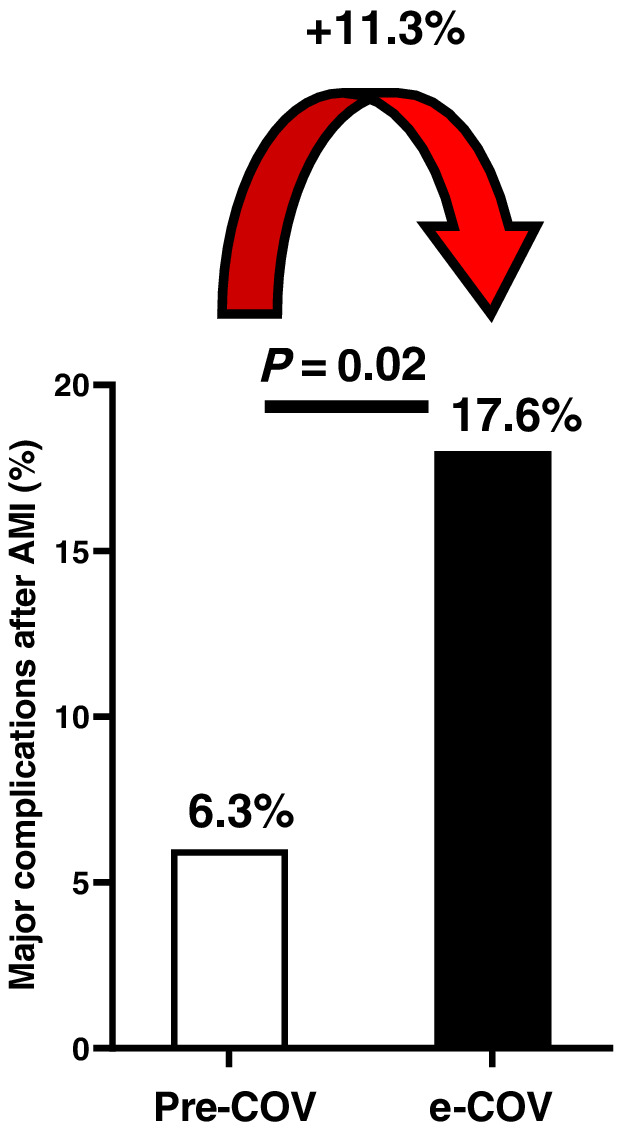
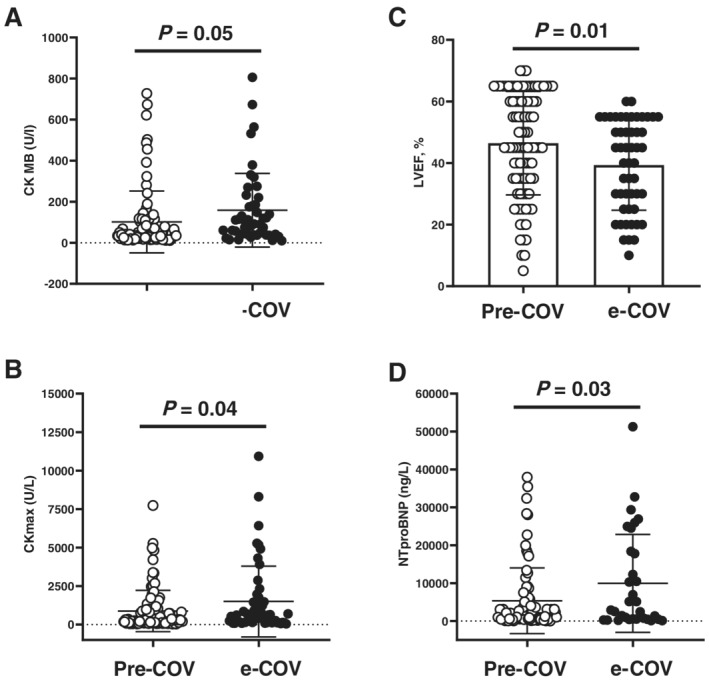
Methods and results: In a single-centre cross-sectional observational study, we included 355 patients with AMI containing ST-elevation or non-ST-elevation myocardial infarction (STEMI or NSTEMI), admitted for emergency cardiac catheterization between January and April 2020 and the equivalent time in 2019. During the early phase of the Covid-19 pandemic (e-COV) in Berlin (March and April 2020), admissions for AMI halved compared with those in the pre-Covid-19 time (January and February 2020; pre-COV) and with those in the corresponding months in 2019. However, mortality for AMI increased substantially from 5.2% pre-COV to 17.7% (P < 0.05) during e-COV. Severity of presentation for AMI was more pronounced during e-COV [increased levels of cardiac enzymes, reduced left ventricular ejection fraction (LVEF), an increase in the need of inotropic support by 25% (P < 0.01)], while patients' demographic and angiographic characteristics did not differ between pre-COV and e-COV. Time from symptom onset to first medical contact was prolonged in all AMI during e-COV (presentation > 72 h +21% in STEMI, p = 0.04 and presentation > 72 h in NSTEMI +22%, p = 0.02). Door to balloon time was similar in STEMI patients, while time from first medical contact to revascularization was significantly delayed in NSTEMI patients (p = 0.02). Major cardiac complications after AMI occurred significantly more often, and cardiac recovery was worse in e-COV than in pre-COV, demonstrated by a significantly lower LVEF (39 ± 16 vs. 46 ± 16, p < 0.05) at hospital discharge and substantially higher NTproBNP levels.
Conclusions: The Covid-19 outbreak affects hospital admissions for acute coronary syndromes. During the first phase of the pandemia, significantly less patients with AMI were admitted, but those admitted presented with a more severe phenotype and had a higher mortality, more complications, and a worse short-term outcome. Therefore, our data indicate that Covid-19 had relevant impact on non-infectious disease states, such as acute coronary syndromes.
Keywords: Acute myocardial infarction; Covid-19; NSTEMI; Percutaneous coronary intervention; SARS-CoV-2; STEMI.
© 2020 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of the European Society of Cardiology.
Conflict of interest statement
The authors declare no conflict of interest in relationship with manuscript content.
Figures
References
-
- Li Q, Guan X, Wu P, Wang X, Zhou L, Tong Y, Ren R, Leung KSM, Lau EHY, Wong JY, Xing X, Xiang N, Wu Y, Li C, Chen Q, Li D, Liu T, Zhao J, Li M, Tu W, Chen C, Jin L, Yang R, Wang Q, Zhou S, Wang R, Liu H, Luo Y, Liu Y, Shao G, Li H, Tao Z, Yang Y, Deng Z, Liu B, Ma Z, Zhang Y, Shi G, Lam TTY, Wu JTK, Gao GF, Cowling BJ, Yang B, Leung GM, Feng Z. Early transmission dynamics in Wuhan, China, of novel coronavirus‐infected pneumonia. N Engl J Med 2020; 382: 1199–1207. - PMC - PubMed
-
- Guan WJ, Ni ZY, Hu Y, Liang WH, Ou CQ, He JX, Liu L, Shan H, Lei CL, Hui DSC, Du B, Li LJ, Zeng G, Yuen KY, Chen RC, Tang CL, Wang T, Chen PY, Xiang J, Li SY, Wang JL, Liang ZJ, Peng YX, Wei L, Liu Y, Hu YH, Peng P, Wang JM, Liu JY, Chen Z, Li G, Zheng ZJ, Qiu SQ, Luo J, Ye CJ, Zhu SY, Zhong NS, China Medical Treatment Expert Group for Covid‐19 . Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med 2020; 382: 1708–1720. - PMC - PubMed
-
- https://covid19.who.int. Accessed date June 19 2020.
-
- Onder G, Rezza G, Brusaferro S. Case‐fatality rate and characteristics of patients dying in relation to COVID‐19 in Italy. JAMA 2020; 323: 1775–1776. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
