

Bilirubin as a metabolic hormone: the physiological relevance of low levels
- PMID: 33284088
- PMCID: PMC8260361
- DOI: 10.1152/ajpendo.00405.2020
Bilirubin as a metabolic hormone: the physiological relevance of low levels
Abstract
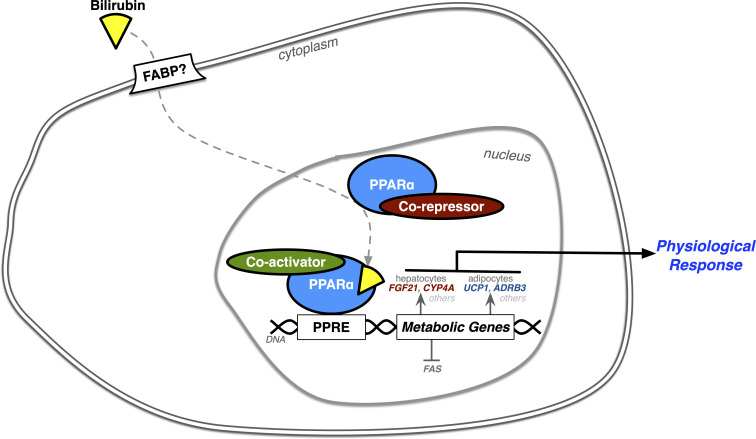
Recent research on bilirubin, a historically well-known waste product of heme catabolism, suggests an entirely new function as a metabolic hormone that drives gene transcription by nuclear receptors. Studies are now revealing that low plasma bilirubin levels, defined as "hypobilirubinemia," are a possible new pathology analogous to the other end of the spectrum of extreme hyperbilirubinemia seen in patients with jaundice and liver dysfunction. Hypobilirubinemia is most commonly seen in patients with metabolic dysfunction, which may lead to cardiovascular complications and possibly stroke. We address the clinical significance of low bilirubin levels. A better understanding of bilirubin's hormonal function may explain why hypobilirubinemia might be deleterious. We present mechanisms by which bilirubin may be protective at mildly elevated levels and research directions that could generate treatment possibilities for patients with hypobilirubinemia, such as targeting of pathways that regulate its production or turnover or the newly designed bilirubin nanoparticles. Our review here calls for a shift in the perspective of an old molecule that could benefit millions of patients with hypobilirubinemia.
Keywords: HO-1; PPARalpha; bilirubin nanoparticles; heme oxygenase; hypobilirubinemia.
Conflict of interest statement
T.D.H. and D.E.S. have submitted patents on bilirubin and obesity related disorders. The other authors have nothing to declare.
Figures






References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical