

Attributable Mortality of Ventilator-associated Pneumonia. Replicating Findings, Revisiting Methods
- PMID: 33285078
- PMCID: PMC8086531
- DOI: 10.1513/AnnalsATS.202004-385OC
Attributable Mortality of Ventilator-associated Pneumonia. Replicating Findings, Revisiting Methods
Abstract
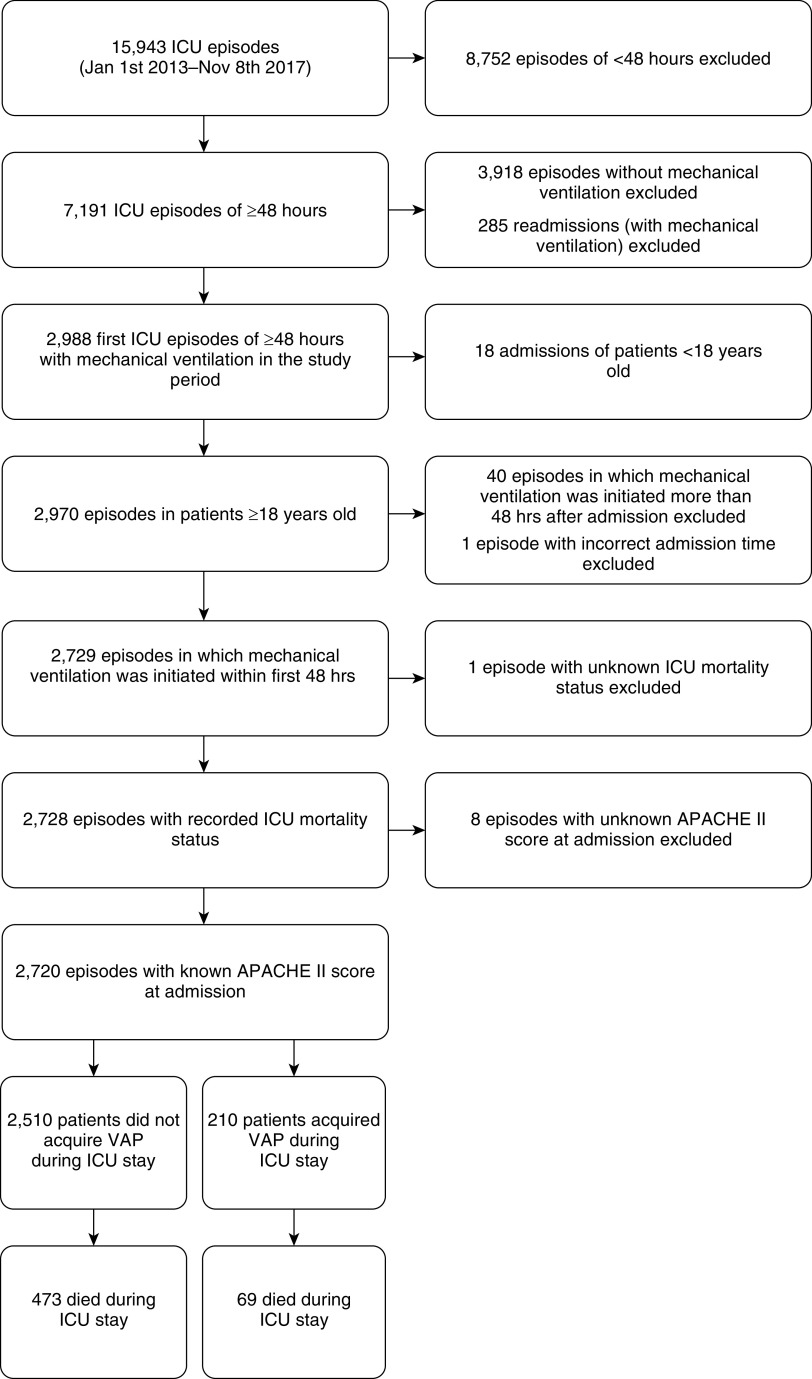
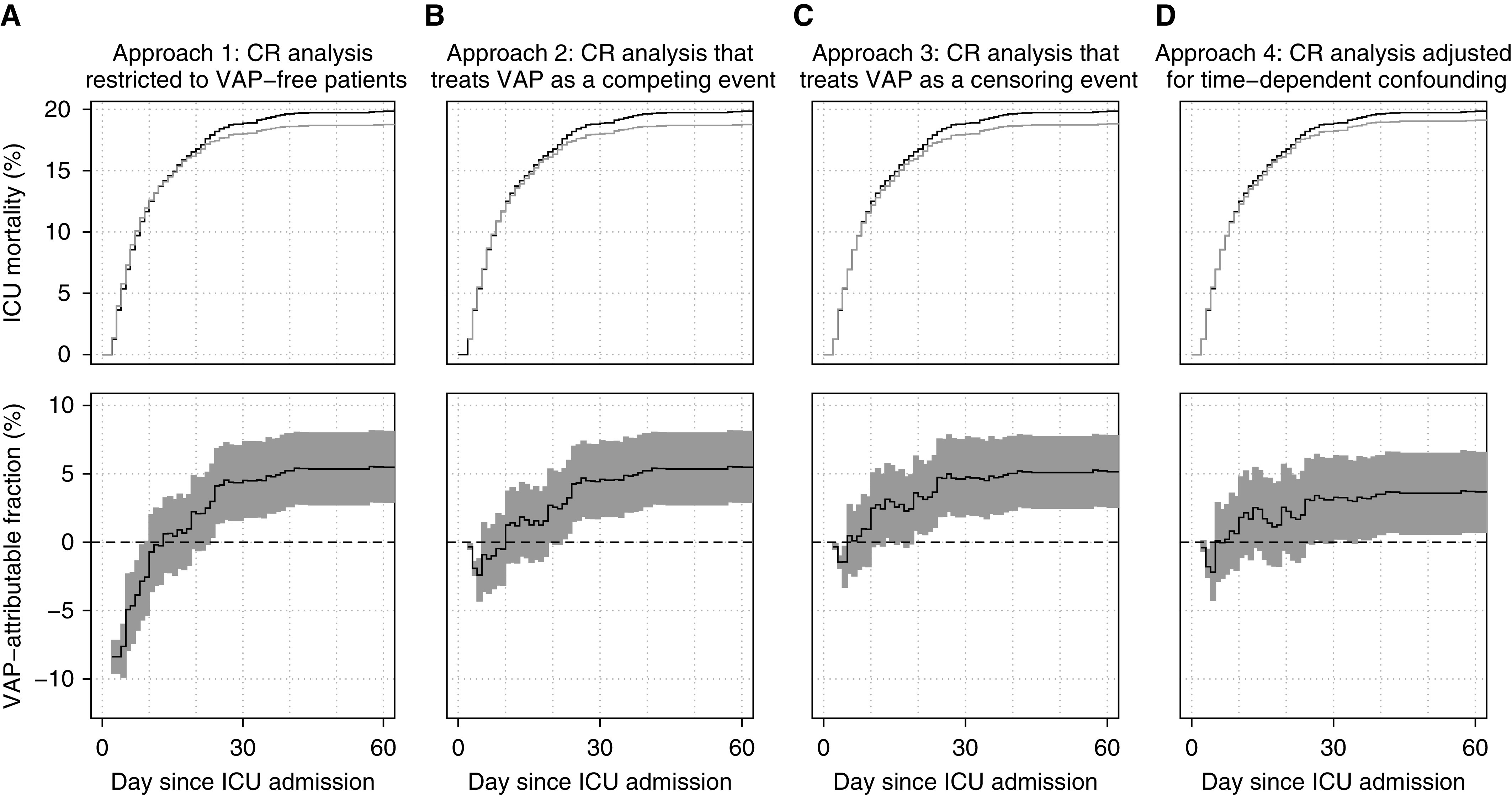
Rationale: Estimating the impact of ventilator-associated pneumonia (VAP) from routinely collected intensive care unit (ICU) data is methodologically challenging.Objectives: We aim to replicate earlier findings of limited VAP-attributable ICU mortality in an independent cohort. By refining statistical analyses, we gradually tackle different sources of bias.Methods: Records of 2,720 adult patients admitted to Ghent University Hospital ICUs (2013-2017) and receiving mechanical ventilation within 48 hours after admission were extracted from linked Intensive Care Information System and Computer-based Surveillance and Alerting of Nosocomial Infections, Antimicrobial Resistance, and Antibiotic Consumption in the ICU databases. The VAP-attributable fraction of ICU mortality was estimated using a competing risk analysis that is restricted to VAP-free patients (approach 1), accounts for VAP onset by treating it as either a competing (approach 2) or censoring event (approach 3), or additionally adjusts for time-dependent confounding via inverse probability weighting (approach 4).Results: A total of 210 patients (7.7%) acquired VAP. Based on benchmark approach 4, we estimated that (compared with current preventive measures) hypothetical eradication of VAP would lead to a relative ICU mortality reduction of 1.7% (95% confidence interval, -1.3 to 4.6) by Day 10 and of 3.6% (95% confidence interval, 0.7 to 6.5) by Day 60. Approaches 1-3 produced estimates ranging from -0.7% to 2.5% by Day 10 and from 5.2% to 5.5% by Day 60.Conclusions: In line with previous studies using appropriate methodology, we found limited VAP-attributable ICU mortality given current state-of-the-art VAP prevention measures. Our study illustrates that inappropriate accounting of the time dependency of exposure and confounding of its effects may misleadingly suggest protective effects of early-onset VAP and systematically overestimate attributable mortality.
Keywords: causality; confounding factors (epidemiology); hospital mortality; survival analysis; ventilator-associated pneumonia.
Figures
Comment in
-
Accurately Measuring Preventable Ventilator-associated Pneumonia Deaths Using Observational Data: It's about Time.Ann Am Thorac Soc. 2021 May;18(5):777-779. doi: 10.1513/AnnalsATS.202102-126ED. Ann Am Thorac Soc. 2021. PMID: 33929311 Free PMC article. No abstract available.
References
-
- Graves N, Weinhold D, Tong E, Birrell F, Doidge S, Ramritu P, et al. Effect of healthcare-acquired infection on length of hospital stay and cost. Infect Control Hosp Epidemiol. 2007;28:280–292. - PubMed
-
- De Angelis G, Murthy A, Beyersmann J, Harbarth S. Estimating the impact of healthcare-associated infections on length of stay and costs. Clin Microbiol Infect. 2010;16:1729–1735. - PubMed
-
- Zimlichman E, Henderson D, Tamir O, Franz C, Song P, Yamin CK, et al. Health care-associated infections: a meta-analysis of costs and financial impact on the US health care system. JAMA Intern Med. 2013;173:2039–2046. - PubMed
-
- Melsen WG, Rovers MM, Koeman M, Bonten MJM. Estimating the attributable mortality of ventilator-associated pneumonia from randomized prevention studies. Crit Care Med. 2011;39:2736–2742. - PubMed
-
- Timsit J-F, Zahar J-R, Chevret S. Attributable mortality of ventilator-associated pneumonia. Curr Opin Crit Care. 2011;17:464–471. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
