

CNS Invasion in Meningioma-How the Intraoperative Assessment Can Improve the Prognostic Evaluation of Tumor Recurrence
- PMID: 33287241
- PMCID: PMC7761660
- DOI: 10.3390/cancers12123620
CNS Invasion in Meningioma-How the Intraoperative Assessment Can Improve the Prognostic Evaluation of Tumor Recurrence
Abstract
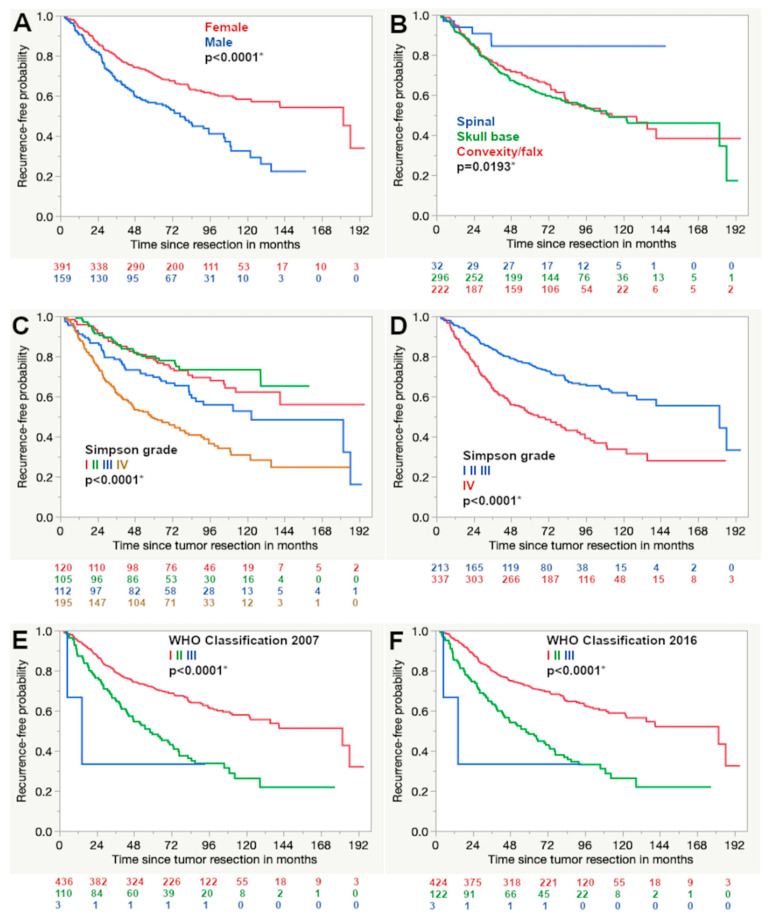
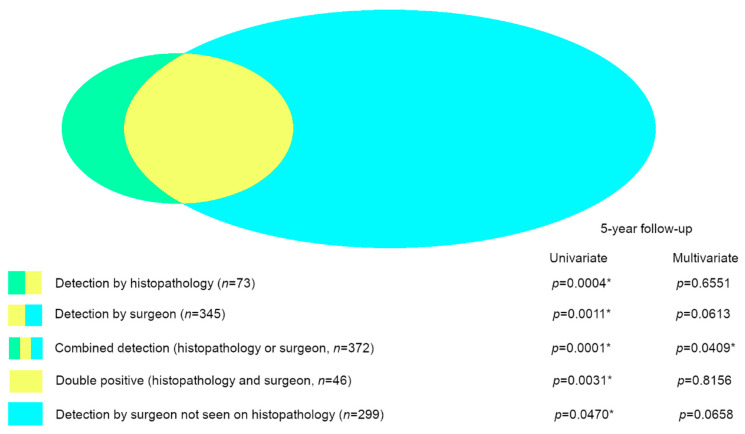
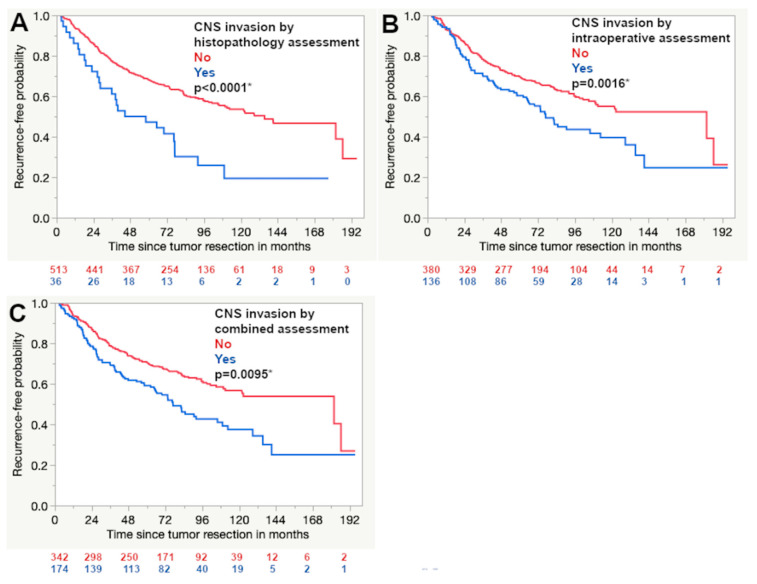
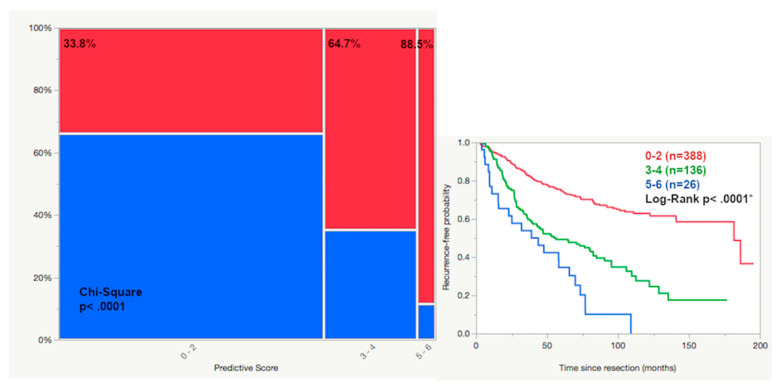
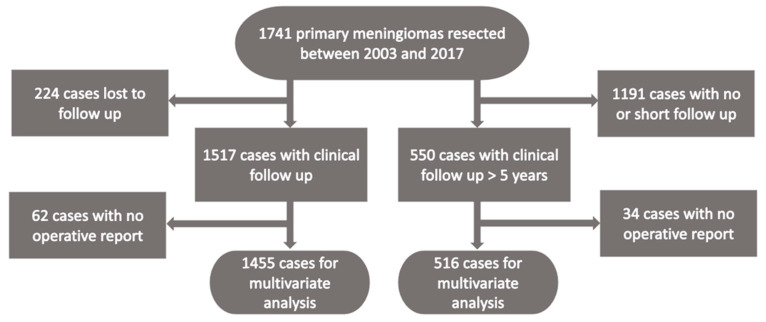
The detection of the infiltrative growth of meningiomas into CNS tissue has been integrated into the WHO classification as a stand-alone marker for atypical meningioma. However, its prognostic impact has been questioned. Infiltrative growth can also be detected intraoperatively. The prognostic impact of the intraoperative detection of the central nervous system tissue invasion of meningiomas was analyzed and compared to the histopathological assessment. The clinical data of 1517 cases with follow-up data regarding radiographic recurrence was collected. Histopathology and operative reports were reviewed and invasive growth was seen during resection in 23.7% (n = 345) while histopathology detected it in 4.8% (n = 73). The histopathological and intraoperative assessments were compatible in 63%. The prognostic impact of histopathological and intraoperative assessment was significant in the univariate but not in the multivariate analysis. Both methods of assessment combined reached statistical significance in the multivariate analysis (p = 0.0409). A score including all independent prognostic factors divided the cohort into three prognostic subgroups with a risk of recurrence of 33.8, 64.7 and 88.5%, respectively. The intraoperative detection of the infiltrative growth of primary meningiomas into the central nervous system tissue can complement the histopathological assessment of CNS invasion. The combined assessment is an independent prognostic factor regarding tumor recurrence and allows a risk-adapted tumor stratification.
Keywords: CNS invasion; brain invasion; intraoperative assessment; invasive growth; meningioma; progression-free survival; recurrence risk.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Louis D.N., Perry A., Reifenberger G., von Deimling A., Figarella-Branger D., Cavenee W.K., Ohgaki H., Wiestler O.D., Kleihues P., Ellison D.W. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: A summary. Acta Neuropathol. 2016;131:803–820. doi: 10.1007/s00401-016-1545-1. - DOI - PubMed
LinkOut - more resources
Full Text Sources
