

Effect of arthroscopic acromioplasty on reducing critical shoulder angle: a protocol for a prospective randomized clinical trial
- PMID: 33287773
- PMCID: PMC7722311
- DOI: 10.1186/s12891-020-03818-w
Effect of arthroscopic acromioplasty on reducing critical shoulder angle: a protocol for a prospective randomized clinical trial
Abstract
Background: The critical shoulder angle (CSA), which helps to predict patients who are at risk of rotator cuff tears (RCTs) with large degree and who are susceptible to osteoarthritis with low angle, has been identified as one of the most vital acromial parameters; anterolateral and lateral acromioplasties have been proven to be valid ways to reduce CSA. However, no study has compared the effect of different acromioplasties on the reduction of the large CSA (≥33°) clinically. Additionally, either anterolateral or lateral acromioplasty could not precisely correct large CSAs to a favorable range (30-33°) in each patient. Thus, we will propose a novel precise acromioplasty technique for the purpose of reducing CSA accurately and effectively, and compare the effectiveness of different acromioplasties on the reduction of the CSA.
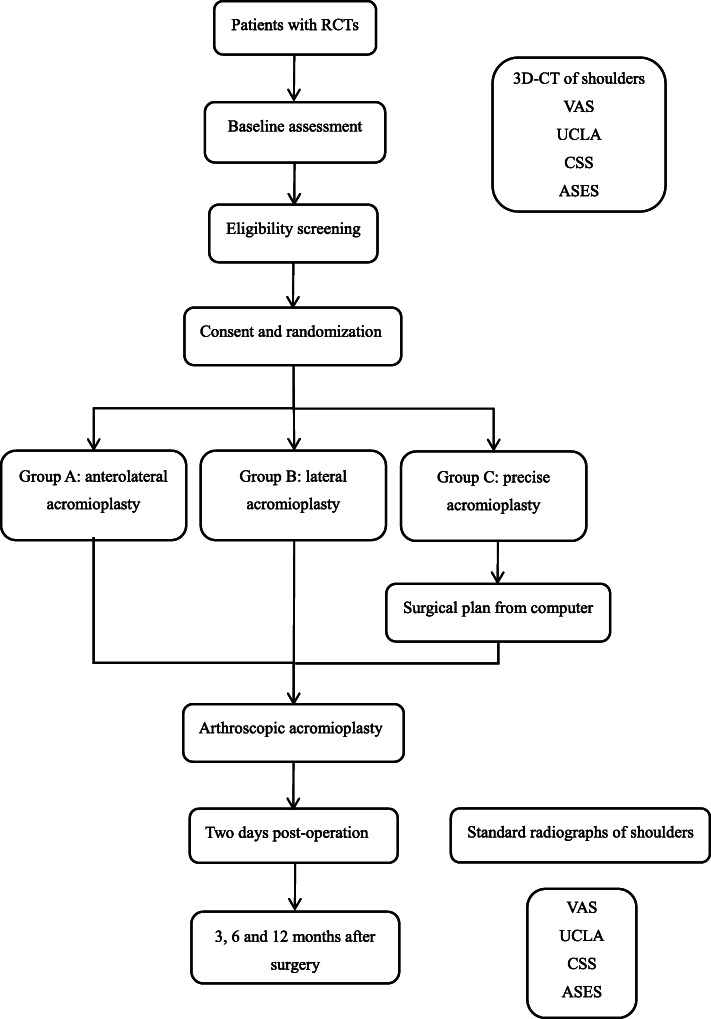
Methods: A total of 60 RCT patients who have indications for arthroscopic rotator cuff repair and with pre-operative CSA ≥33° will be recruited in outpatient center of Sun Yat-sen Memorial Hospital. Eligible participants will be randomly allocated to Group A (anterolateral acromioplasty), Group B (lateral acromioplasty) or Group C (precise acromioplasty) via a random, computer-generated number system. Three surgical plans will be made for each participant respectively by one professional surgeon according to the results of randomization allocation. The post-operative CSA will be measured 2 days post-operation. Follow-up will be maintained at 3, 6, and 12 months after surgery including the visual analog scale score, the University of California at Los Angeles score, the Constant Shoulder Score and the American Shoulder and Elbow Surgeon Shoulder Assessment Form. Finally, all outcomes will be assessed by two researchers who are blinded to the recruitment and allocation.
Discussion: This is the first clinical trial to evaluate the impact of different acromioplasties on the reduction of the CSA. Additionally, this study will provide a new precise acromioplasty technique, which is a novel precision and individualized treatment to prevent degenerative RCTs by reducing the CSA.
Trial registration: ChiCTR2000032343 . Registered on April 26th, 2020.
Keywords: 3D reconstruction; Acromioplasty; Critical shoulder angle; Rotator cuff tears.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
