

Imaging of COVID-19: CT, MRI, and PET
- PMID: 33288215
- PMCID: PMC7703471
- DOI: 10.1053/j.semnuclmed.2020.11.003
Imaging of COVID-19: CT, MRI, and PET
Abstract
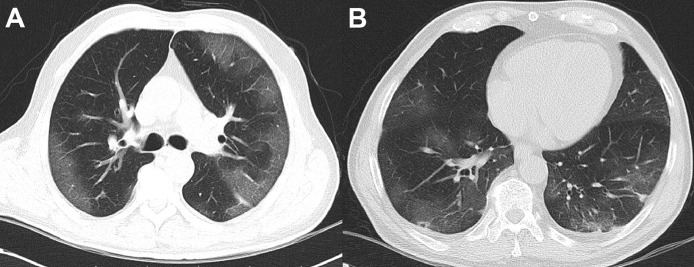
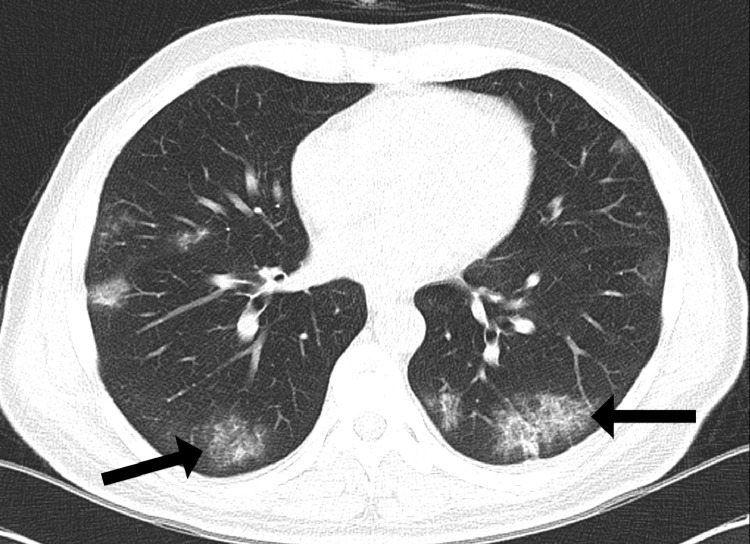
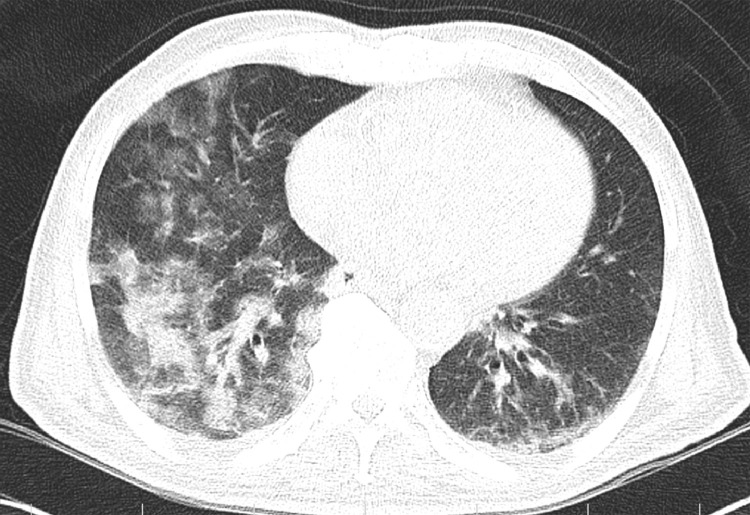
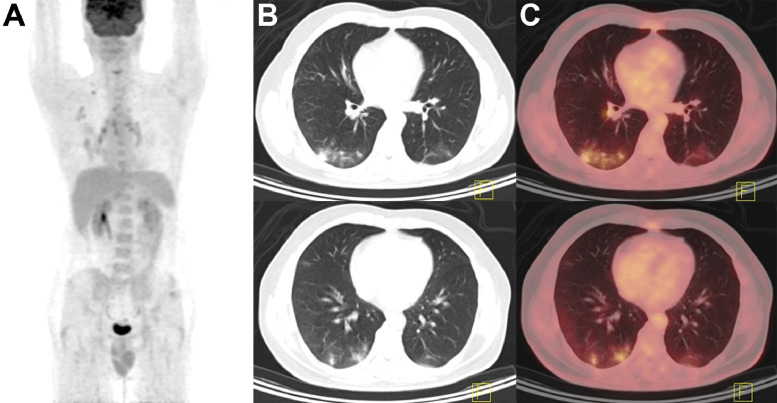
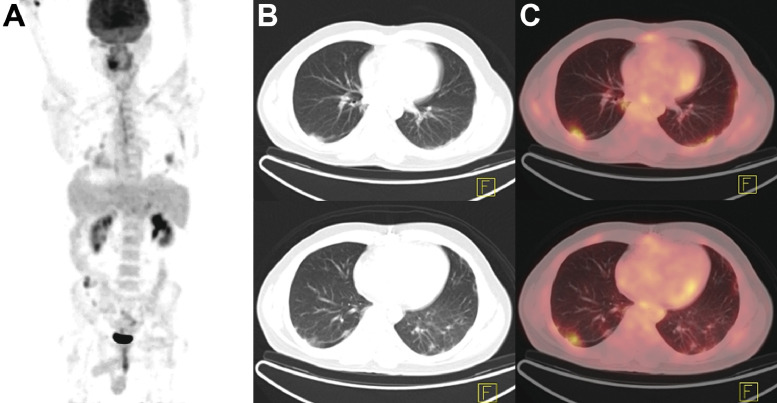
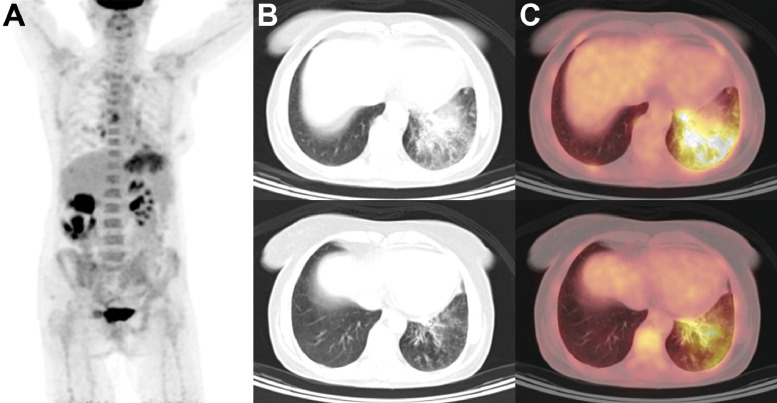
Soon after reports of a novel coronavirus capable of causing severe pneumonia surfaced in late 2019, expeditious global spread of the Severe Acute Respiratory Distress Syndrome Coronavirus 2 (SARS-CoV-2) forced the World Health Organization to declare an international state of emergency. Although best known for causing symptoms of upper respiratory tract infection in mild cases and fulminant pneumonia in severe disease, Coronavirus Disease 2019 (COVID-19) has also been associated with gastrointestinal, neurologic, cardiac, and hematologic presentations. Despite concerns over poor specificity and undue radiation exposure, chest imaging nonetheless remains central to the initial diagnosis and monitoring of COVID-19 progression, as well as to the evaluation of complications. Classic features on chest CT include ground-glass and reticular opacities with or without superimposed consolidations, frequently presenting in a bilateral, peripheral, and posterior distribution. More recently, studies conducted with MRI have shown excellent concordance with chest CT in visualizing typical features of COVID-19 pneumonia. For patients in whom exposure to ionizing radiation should be avoided, particularly pregnant patients and children, pulmonary MRI may represent a suitable alternative to chest CT. Although PET imaging is not typically considered among first-line investigative modalities for the diagnosis of lower respiratory tract infections, numerous reports have noted incidental localization of radiotracer in parenchymal regions of COVID-19-associated pulmonary lesions. These findings are consistent with data from Middle East Respiratory Syndrome-CoV cohorts which suggested an ability for 18F-FDG PET to detect subclinical infection and lymphadenitis in subjects without overt clinical signs of infection. Though highly sensitive, use of PET/CT for primary detection of COVID-19 is constrained by poor specificity, as well as considerations of cost, radiation burden, and prolonged exposure times for imaging staff. Even still, decontamination of scanner bays is a time-consuming process, and proper ventilation of scanner suites may additionally require up to an hour of downtime to allow for sufficient air exchange. Yet, in patients who require nuclear medicine investigations for other clinical indications, PET imaging may yield the earliest detection of nascent infection in otherwise asymptomatic individuals. Especially for patients with concomitant malignancies and other states of immunocompromise, prompt recognition of infection and early initiation of supportive care is crucial to maximizing outcomes and improving survivability.
Copyright © 2020 Elsevier Inc. All rights reserved.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
