

Calcium cytotoxicity sensitizes prostate cancer cells to standard-of-care treatments for locally advanced tumors
- PMID: 33288740
- PMCID: PMC7721710
- DOI: 10.1038/s41419-020-03256-5
Calcium cytotoxicity sensitizes prostate cancer cells to standard-of-care treatments for locally advanced tumors
Abstract
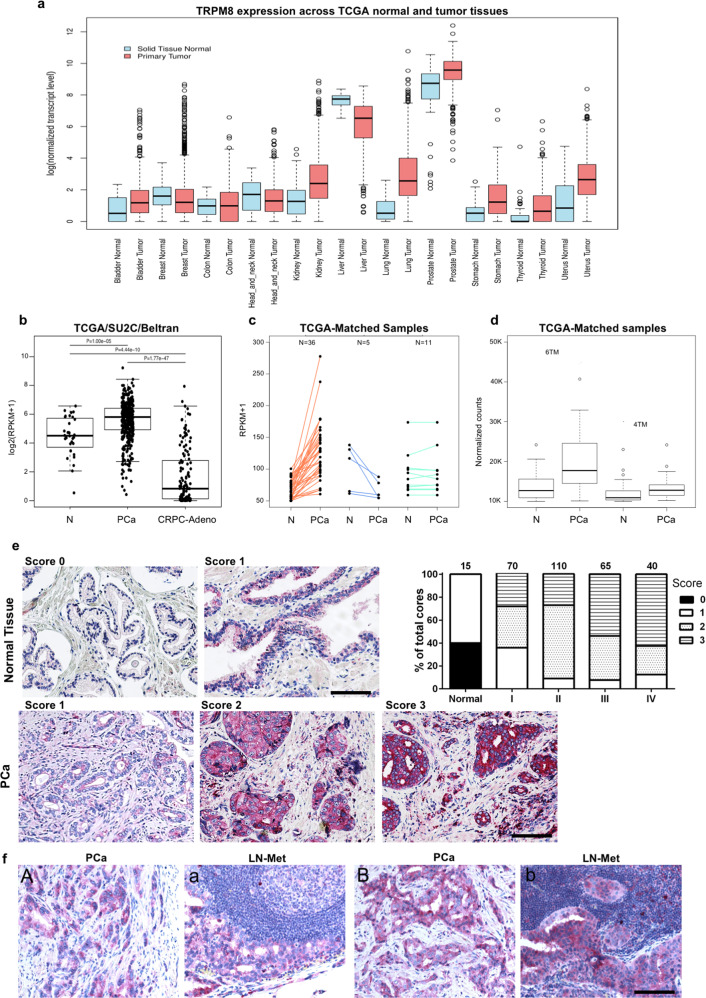
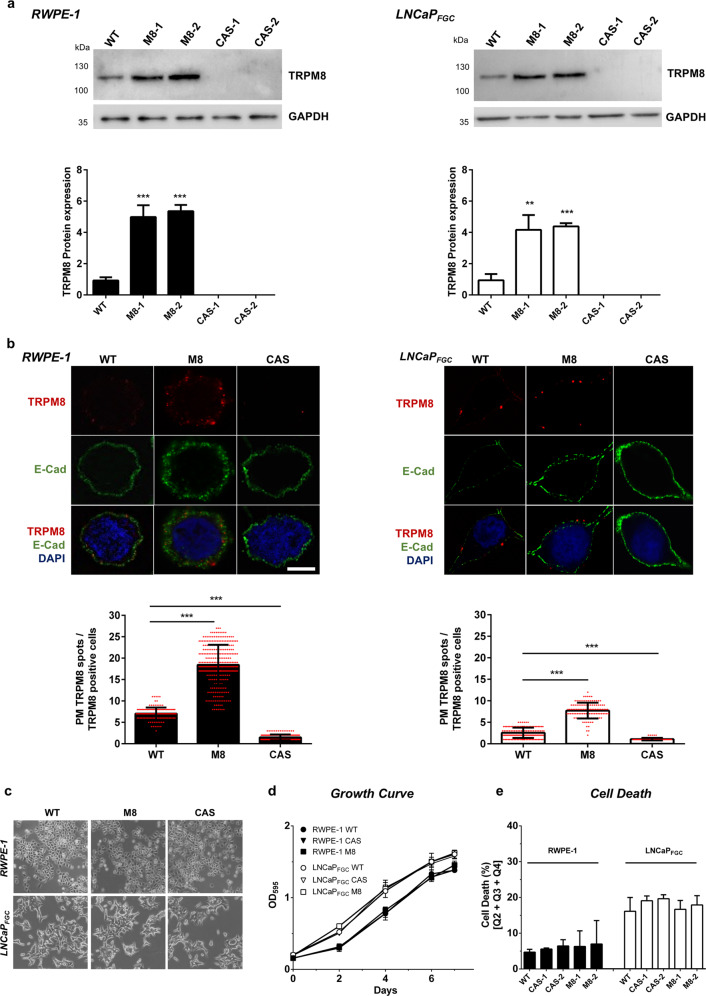
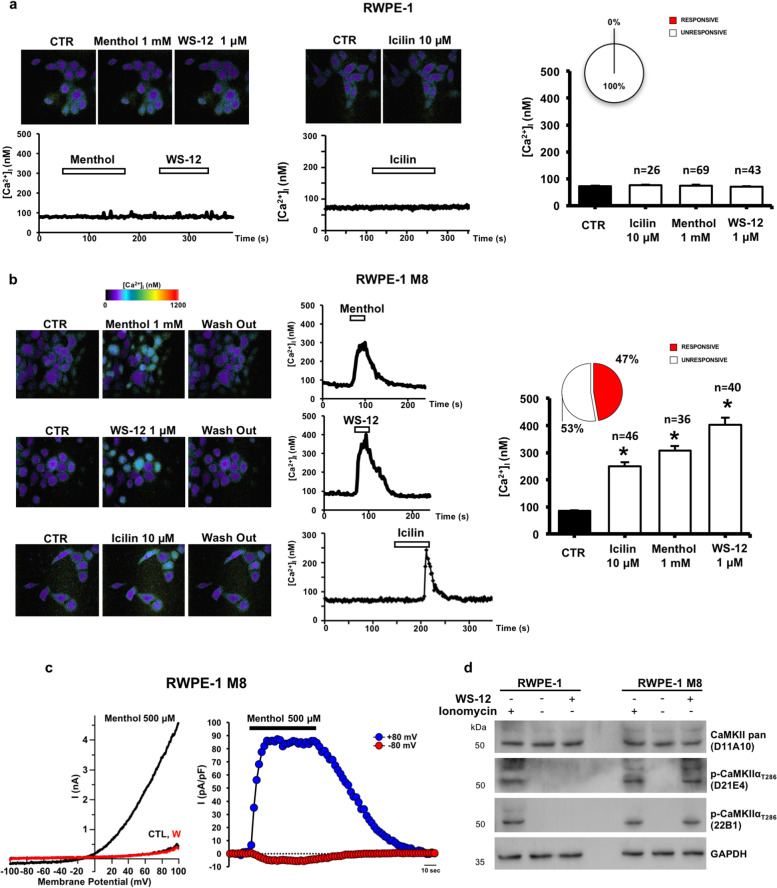
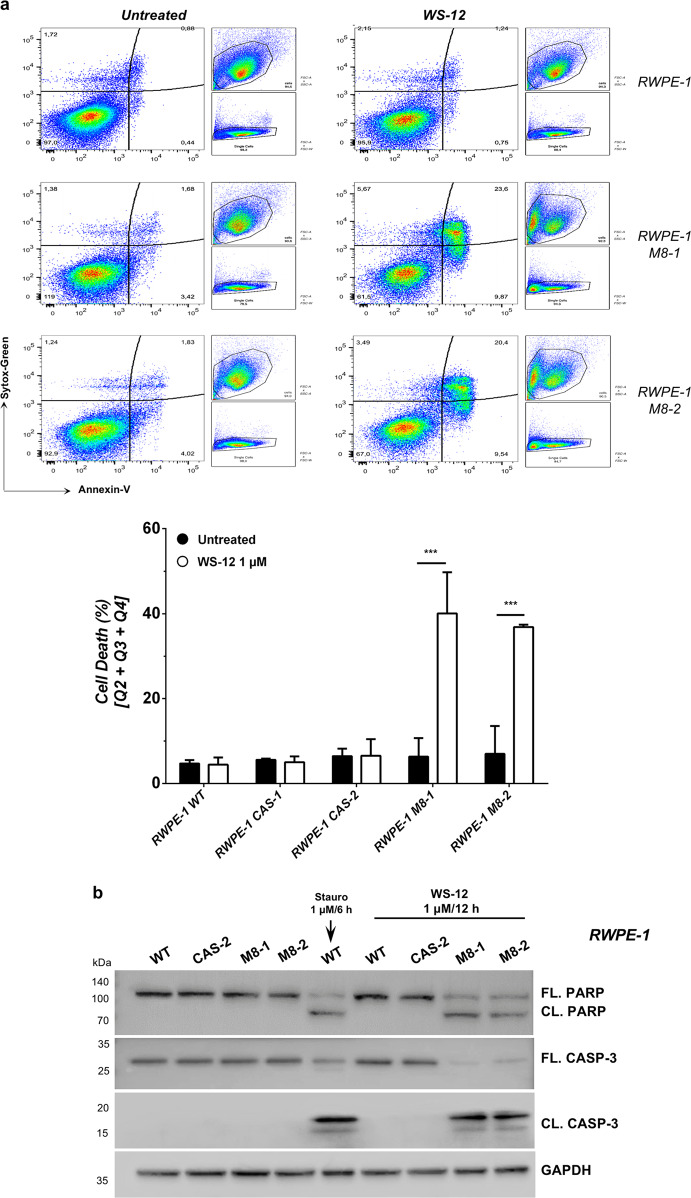
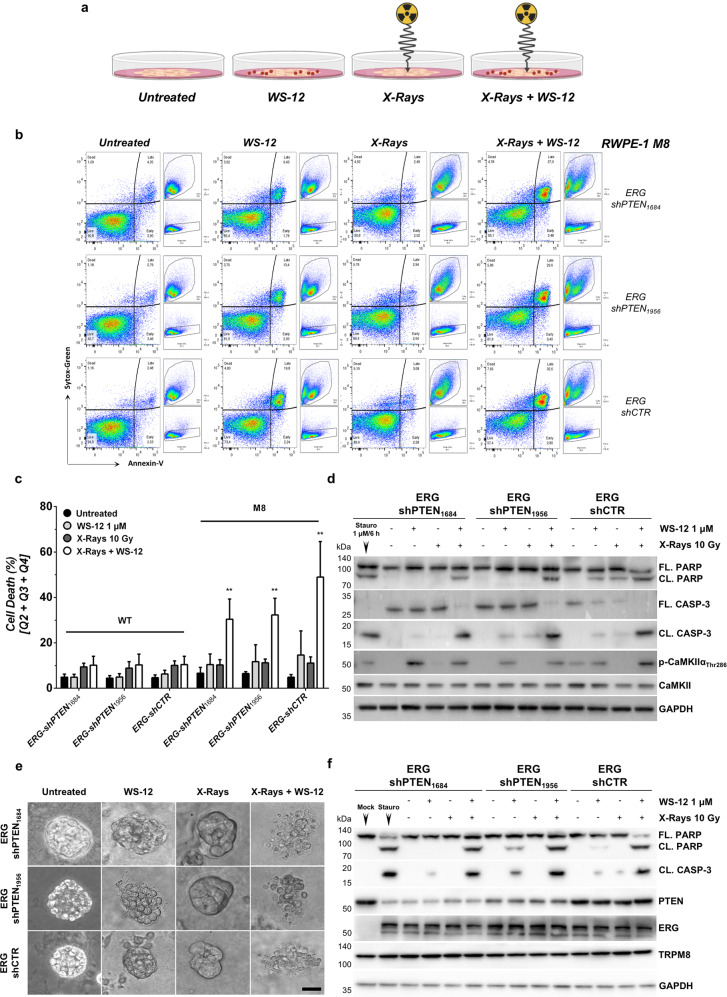
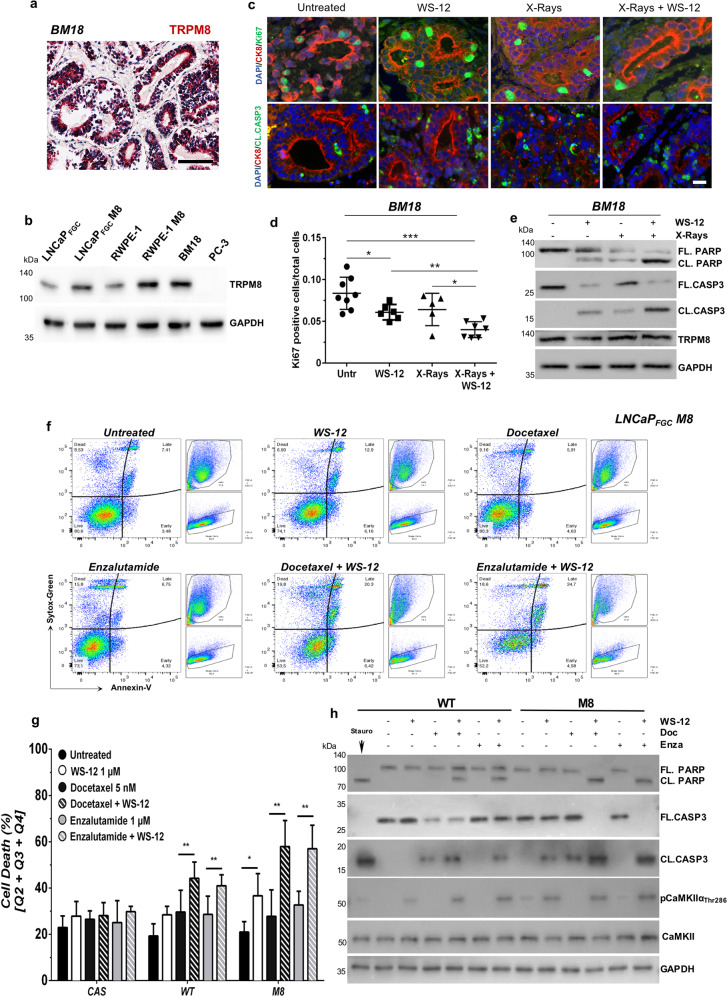
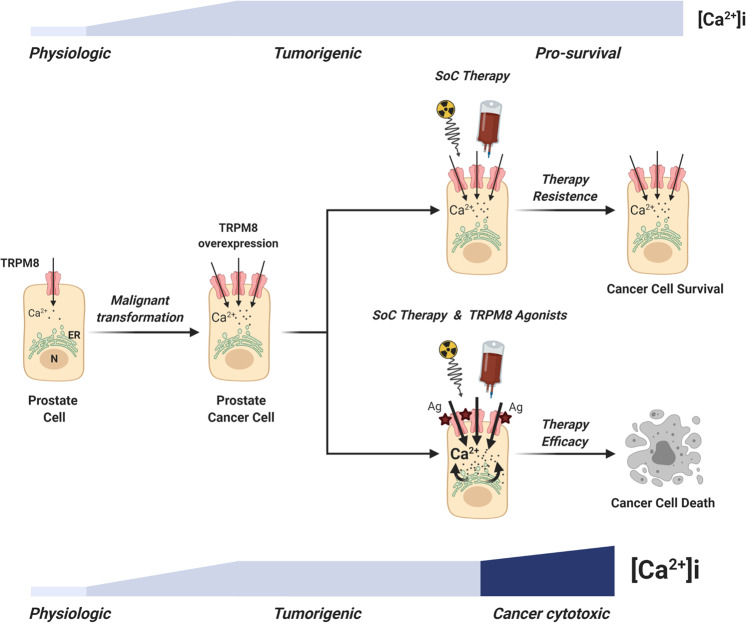
Therapy resistance is a major roadblock in oncology. Exacerbation of molecular dysfunctions typical of cancer cells have proven effective in twisting oncogenic mechanisms to lethal conditions, thus offering new therapeutic avenues for cancer treatment. Here, we demonstrate that selective agonists of Transient Receptor Potential cation channel subfamily M member 8 (TRPM8), a cation channel characteristic of the prostate epithelium frequently overexpressed in advanced stage III/IV prostate cancers (PCa), sensitize therapy refractory models of PCa to radio, chemo or hormonal treatment. Overall, our study demonstrates that pharmacological-induced Ca2+ cytotoxicity is an actionable strategy to sensitize cancer cells to standard therapies.
Conflict of interest statement
A.C. and G.P. are cofounders and scientific advisors of Alia Therapeutics. The other authors disclosed no potential conflicts of interest.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
