

Proceedings of the Comprehensive Oncology Network Evaluating Rare CNS Tumors (NCI-CONNECT) Oligodendroglioma Workshop
- PMID: 33289010
- PMCID: PMC7212866
- DOI: 10.1093/noajnl/vdz048
Proceedings of the Comprehensive Oncology Network Evaluating Rare CNS Tumors (NCI-CONNECT) Oligodendroglioma Workshop
Abstract
Background: Oligodendroglioma is a rare primary central nervous system (CNS) tumor with highly variable outcome and for which therapy is usually not curative. At present, little is known regarding the pathways involved with progression of oligodendrogliomas or optimal biomarkers for stratifying risk. Developing new therapies for this rare cancer is especially challenging. To overcome these challenges, the neuro-oncology community must be particularly innovative, seeking multi-institutional and international collaborations, and establishing partnerships with patients and advocacy groups thereby ensuring that each patient enrolled in a study is as informative as possible.
Methods: The mission of the National Cancer Institute's NCI-CONNECT program is to address the challenges and unmet needs in rare CNS cancer research and treatment by connecting patients, health care providers, researchers, and advocacy organizations to work in partnership. On November 19, 2018, the program convened a workshop on oligodendroglioma, one of the 12 rare CNS cancers included in its initial portfolio. The purpose of this workshop was to discuss scientific progress and regulatory challenges in oligodendroglioma research and develop a call to action to advance research and treatment for this cancer.
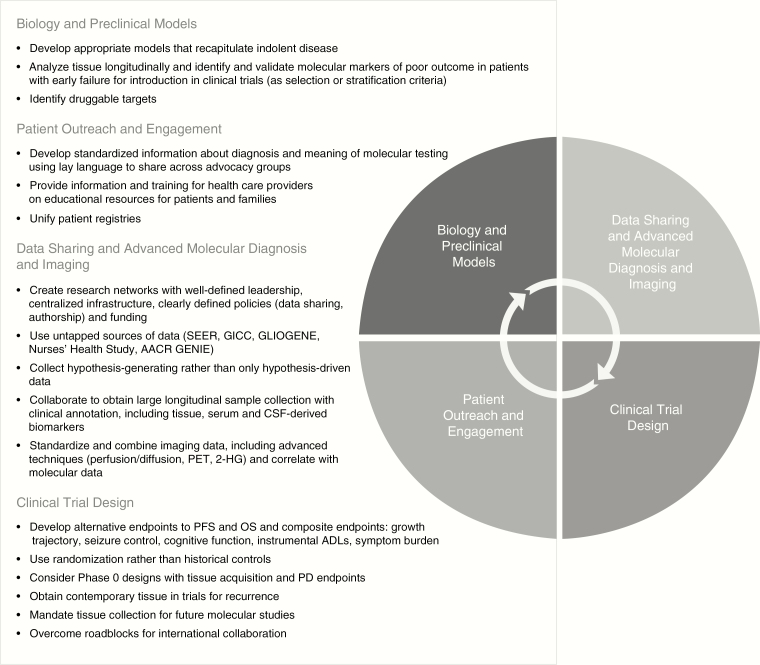
Results: The recommendations of the workshop include a multifaceted and interrelated approach covering: biology and preclinical models, data sharing and advanced molecular diagnosis and imaging; clinical trial design; and patient outreach and engagement.
Conclusions: The NCI-CONNECT program is well positioned to address challenges in oligodendroglioma care and research in collaboration with other stakeholders and is developing a list of action items for future initiatives.
Keywords: NCI-CONNECT; oligodendroglioma; rare CNS tumors; workshop.
© Published by Oxford University Press on behalf of the Society for Neuro-Oncology and the European Association of Neuro-Oncology 2019.
Figures
References
-
- Louis DN, Perry A, Reifenberger G, et al. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: a summary. Acta Neuropathol. 2016;131(6):803–820. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous