

Immune Checkpoint Inhibitor with or without Radiotherapy in Melanoma Patients with Brain Metastases: A Systematic Review and Meta-Analysis
- PMID: 33289357
- PMCID: PMC8005357
- DOI: 10.3348/kjr.2020.0728
Immune Checkpoint Inhibitor with or without Radiotherapy in Melanoma Patients with Brain Metastases: A Systematic Review and Meta-Analysis
Abstract
Objective: Immune checkpoint inhibitor (ICI) therapy has shown activity against melanoma brain metastases. Recently, promising results have also been reported for ICI combination therapy and ICI combined with radiotherapy. We aimed to evaluate radiologic response and adverse event rates of these therapeutic options by a systematic review and meta-analysis.
Materials and methods: A systematic literature search of Ovid-MEDLINE and EMBASE was performed up to October 12, 2019 and included studies evaluating the intracranial objective response rates (ORRs) and/or disease control rates (DCRs) of ICI with or without radiotherapy for treating melanoma brain metastases. We also evaluated safety-associated outcomes.
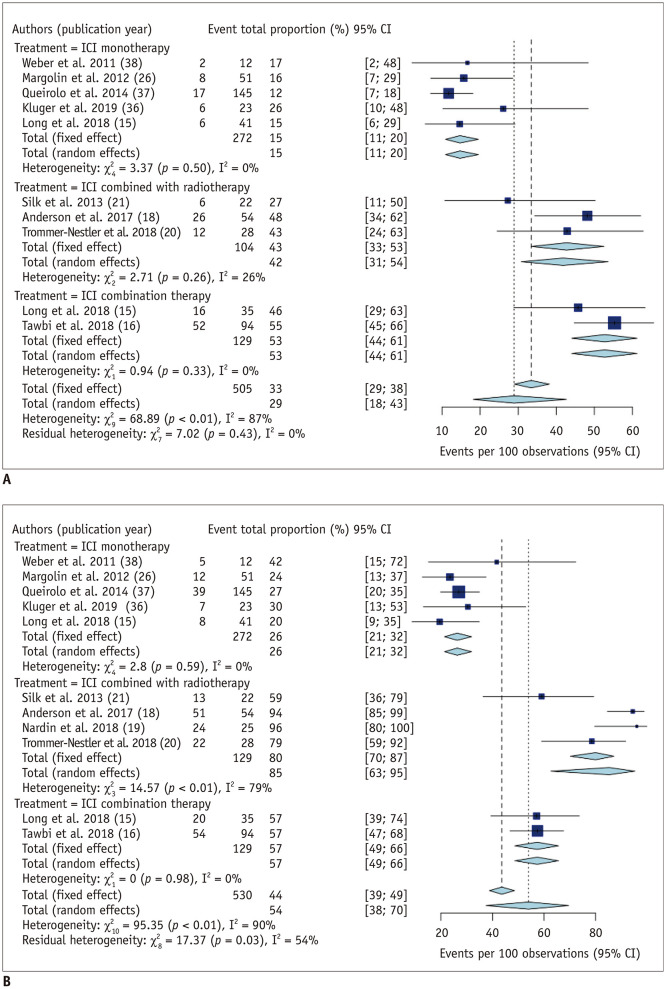
Results: Eleven studies with 14 cohorts (3 with ICI combination therapy; 5 with ICI combined with radiotherapy; 6 with ICI monotherapy) were included. ICI combination therapy {pooled ORR, 53% (95% confidence interval [CI], 44-61%); DCR, 57% (95% CI, 49-66%)} and ICI combined with radiotherapy (pooled ORR, 42% [95% CI, 31-54%]; DCR, 85% [95% CI, 63-95%]) showed higher local efficacy compared to ICI monotherapy (pooled ORR, 15% [95% CI, 11-20%]; DCR, 26% [95% CI, 21-32%]). The grade 3 or 4 adverse event rate was significantly higher with ICI combination therapy (60%; 95% CI, 52-67%) compared to ICI monotherapy (11%; 95% CI, 8-17%) and ICI combined with radiotherapy (4%; 95% CI, 1-19%). Grade 3 or 4 central nervous system (CNS)-related adverse event rates were not different (9% in ICI combination therapy; 8% in ICI combined with radiotherapy; 5% in ICI monotherapy).
Conclusion: ICI combination therapy or ICI combined with radiotherapy showed better local efficacy than ICI monotherapy for treating melanoma brain metastasis. The grade 3 or 4 adverse event rate was highest with ICI combination therapy, and the CNS-related grade 3 or 4 event rate was similar. Prospective trials will be necessary to compare the efficacy of ICI combination therapy and ICI combined with radiotherapy.
Keywords: Immune checkpoint inhibitor; Immunotherapy; Meta-analysis; Radiation; Radiotherapy.
Copyright © 2021 The Korean Society of Radiology.
Conflict of interest statement
The authors have no potential conflicts of interest to disclose.
Figures
References
-
- Sampson JH, Carter JH, Jr, Friedman AH, Seigler HF. Demographics, prognosis, and therapy in 702 patients with brain metastases from malignant melanoma. J Neurosurg. 1998;88:11–20. - PubMed
-
- Amer MH, Al-Sarraf M, Vaitkevicius VK. Clinical presentation, natural history and prognostic factors in advanced malignant melanoma. Surg Gynecol Obstet. 1979;149:687–692. - PubMed
-
- Budman DR, Camacho E, Wittes RE. The current causes of death in patients with malignant melanoma. Eur J Cancer. 1978;14:327–330. - PubMed
-
- Davies MA, Liu P, McIntyre S, Kim KB, Papadopoulos N, Hwu WJ, et al. Prognostic factors for survival in melanoma patients with brain metastases. Cancer. 2011;117:1687–1696. - PubMed
-
- Fife KM, Colman MH, Stevens GN, Firth IC, Moon D, Shannon KF, et al. Determinants of outcome in melanoma patients with cerebral metastases. J Clin Oncol. 2004;22:1293–1300. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
