

Radiomics of Non-Contrast-Enhanced T1 Mapping: Diagnostic and Predictive Performance for Myocardial Injury in Acute ST-Segment-Elevation Myocardial Infarction
- PMID: 33289360
- PMCID: PMC8005349
- DOI: 10.3348/kjr.2019.0969
Radiomics of Non-Contrast-Enhanced T1 Mapping: Diagnostic and Predictive Performance for Myocardial Injury in Acute ST-Segment-Elevation Myocardial Infarction
Abstract
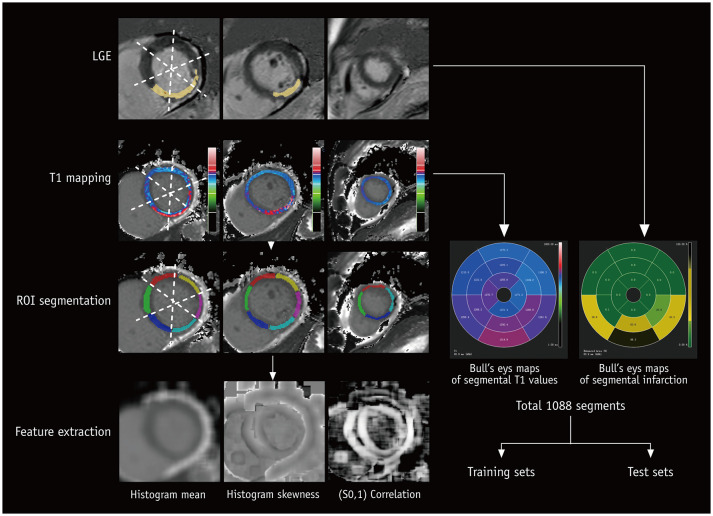
Objective: To evaluate the feasibility of texture analysis on non-contrast-enhanced T1 maps of cardiac magnetic resonance (CMR) imaging for the diagnosis of myocardial injury in acute myocardial infarction (MI).
Materials and methods: This study included 68 patients (57 males and 11 females; mean age, 55.7 ± 10.5 years) with acute ST-segment-elevation MI who had undergone 3T CMR after a percutaneous coronary intervention. Forty patients of them also underwent a 6-month follow-up CMR. The CMR protocol included T2-weighted imaging, T1 mapping, rest first-pass perfusion, and late gadolinium enhancement. Radiomics features were extracted from the T1 maps using open-source software. Radiomics signatures were constructed with the selected strongest features to evaluate the myocardial injury severity and predict the recovery of left ventricular (LV) longitudinal systolic myocardial contractility.
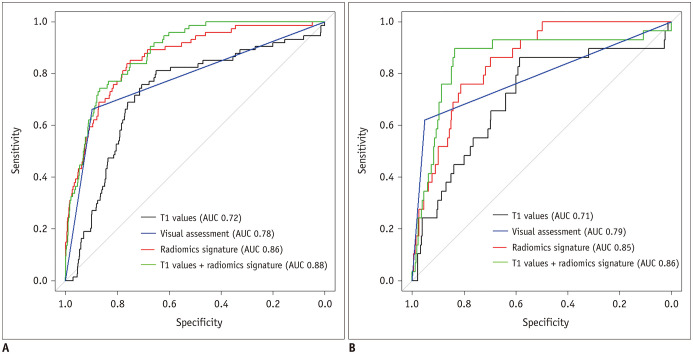
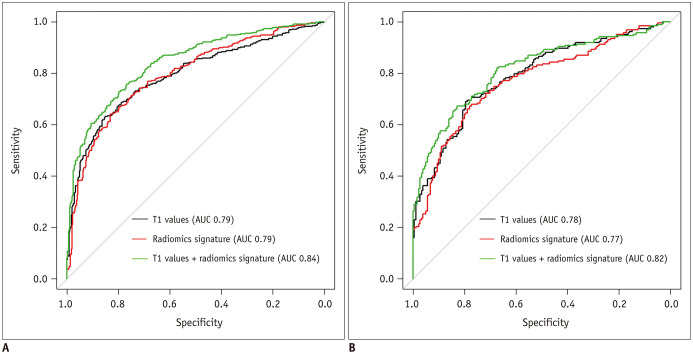
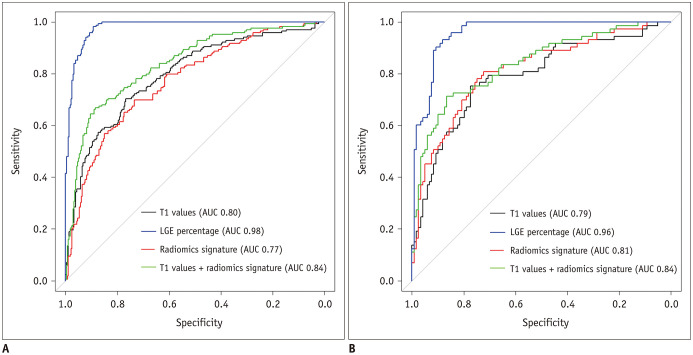
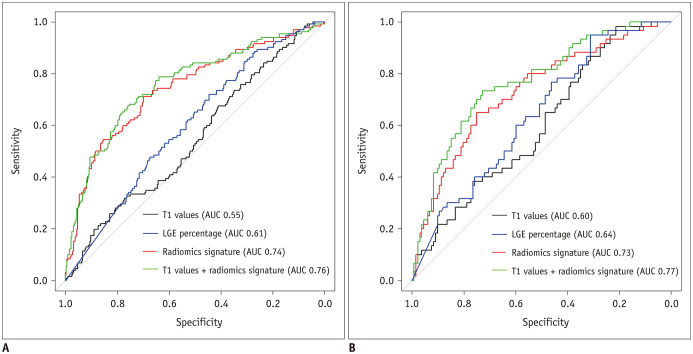
Results: A total of 1088 segments of the acute CMR images were analyzed; 103 (9.5%) segments showed microvascular obstruction (MVO), and 557 (51.2%) segments showed MI. A total of 640 segments were included in the 6-month follow-up analysis, of which 160 (25.0%) segments showed favorable recovery of LV longitudinal systolic myocardial contractility. Combined radiomics signature and T1 values resulted in a higher diagnostic performance for MVO compared to T1 values alone (area under the curve [AUC] in the training set; 0.88, 0.72, p = 0.031: AUC in the test set; 0.86, 0.71, p002). Combined radiomics signature and T1 values also provided a higher predictive value for LV longitudinal systolic myocardial contractility recovery compared to T1 values (AUC in the training set; 0.76, 0.55, p < 0.001: AUC in the test set; 0.77, 0.60, p < 0.001).
Conclusion: The combination of radiomics of non-contrast-enhanced T1 mapping and T1 values could provide higher diagnostic accuracy for MVO. Radiomics also provides incremental value in the prediction of LV longitudinal systolic myocardial contractility at six months.
Keywords: Machine learning; Magnetic resonance imaging; Myocardial infarction; Myocardial reperfusion injury.
Copyright © 2021 The Korean Society of Radiology.
Conflict of interest statement
The authors have no potential conflicts of interest to disclose.
Figures
Similar articles
-
CMR Native T1 Mapping Allows Differentiation of Reversible Versus Irreversible Myocardial Damage in ST-Segment-Elevation Myocardial Infarction: An OxAMI Study (Oxford Acute Myocardial Infarction).Circ Cardiovasc Imaging. 2017 Aug;10(8):e005986. doi: 10.1161/CIRCIMAGING.116.005986. Circ Cardiovasc Imaging. 2017. PMID: 28798137 Free PMC article.
-
Hyper-acute cardiovascular magnetic resonance T1 mapping predicts infarct characteristics in patients with ST elevation myocardial infarction.J Cardiovasc Magn Reson. 2020 Jan 9;22(1):3. doi: 10.1186/s12968-019-0593-9. J Cardiovasc Magn Reson. 2020. PMID: 31915031 Free PMC article.
-
Relationship of Myocardial Strain and Markers of Myocardial Injury to Predict Segmental Recovery After Acute ST-Segment-Elevation Myocardial Infarction.Circ Cardiovasc Imaging. 2016 Jun;9(6):e003457. doi: 10.1161/CIRCIMAGING.115.003457. Circ Cardiovasc Imaging. 2016. PMID: 27283007 Clinical Trial.
-
Machine learning in cardiovascular magnetic resonance: basic concepts and applications.J Cardiovasc Magn Reson. 2019 Oct 7;21(1):61. doi: 10.1186/s12968-019-0575-y. J Cardiovasc Magn Reson. 2019. PMID: 31590664 Free PMC article. Review.
-
T2-weighted cardiovascular magnetic resonance in acute cardiac disease.J Cardiovasc Magn Reson. 2011 Feb 18;13(1):13. doi: 10.1186/1532-429X-13-13. J Cardiovasc Magn Reson. 2011. PMID: 21332972 Free PMC article. Review.
Cited by
-
Development and evaluation of a radiomics model of resting 13N-ammonia positron emission tomography myocardial perfusion imaging to predict coronary artery stenosis in patients with suspected coronary heart disease.Ann Transl Med. 2022 Nov;10(21):1167. doi: 10.21037/atm-22-4692. Ann Transl Med. 2022. PMID: 36467349 Free PMC article.
-
Artificial Intelligence-A Good Assistant to Multi-Modality Imaging in Managing Acute Coronary Syndrome.Front Cardiovasc Med. 2022 Feb 16;8:782971. doi: 10.3389/fcvm.2021.782971. eCollection 2021. Front Cardiovasc Med. 2022. PMID: 35252367 Free PMC article. Review.
-
Native T1 Mapping-Based Radiomics for Noninvasive Prediction of the Therapeutic Effect of Pulmonary Arterial Hypertension.Diagnostics (Basel). 2022 Oct 14;12(10):2492. doi: 10.3390/diagnostics12102492. Diagnostics (Basel). 2022. PMID: 36292180 Free PMC article.
-
Association Between Extracellular Volume Assessed by Cardiac MRI and New-Onset Atrial Fibrillation in Patients With ST-Segment Elevation Myocardial Infarction.Korean J Radiol. 2025 Jun;26(6):546-556. doi: 10.3348/kjr.2025.0070. Korean J Radiol. 2025. PMID: 40432261 Free PMC article.
-
The Road Toward Reproducibility of Parametric Mapping of the Heart: A Technical Review.Front Cardiovasc Med. 2022 May 6;9:876475. doi: 10.3389/fcvm.2022.876475. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 35600490 Free PMC article. Review.
References
-
- Symons R, Masci PG, Goetschalckx K, Doulaptsis K, Janssens S, Bogaert J. Effect of infarct severity on regional and global left ventricular remodeling in patients with successfully reperfused ST segment elevation myocardial infarction. Radiology. 2015;274:93–102. - PubMed
-
- Yamashita Y, Shiomi H, Morimoto T, Yaku H, Furukawa Y, Nakagawa Y, et al. Cardiac and noncardiac causes of long-term mortality in ST-segment-elevation acute myocardial infarction patients who underwent primary percutaneous coronary intervention. Circ Cardiovasc Qual Outcomes. 2017;10:e002790. - PubMed
-
- Dagres N, Hindricks G. Risk stratification after myocardial infarction: is left ventricular ejection fraction enough to prevent sudden cardiac death? Eur Heart J. 2013;34:1964–1971. - PubMed
-
- Masci PG, Pavon AG, Pontone G, Symons R, Lorenzoni V, Francone M, et al. Early or deferred cardiovascular magnetic resonance after ST-segment-elevation myocardial infarction for effective risk stratification. Eur Heart J Cardiovasc Imaging. 2020;21:632–639. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
