

Decision Support Capabilities of Telemedicine in Emergency Prehospital Care: Systematic Review
- PMID: 33289672
- PMCID: PMC7755537
- DOI: 10.2196/18959
Decision Support Capabilities of Telemedicine in Emergency Prehospital Care: Systematic Review
Abstract
Background: Telemedicine offers a unique opportunity to improve coordination and administration for urgent patient care remotely. In an emergency setting, it has been used to support first responders by providing telephone or video consultation with specialists at hospitals and through the exchange of prehospital patient information. This technological solution is evolving rapidly, yet there is a concern that it is being implemented without a demonstrated clinical need and effectiveness as well as without a thorough economic evaluation.
Objective: Our objective is to systematically review whether the clinical outcomes achieved, as reported in the literature, favor telemedicine decision support for medical interventions during prehospital care.
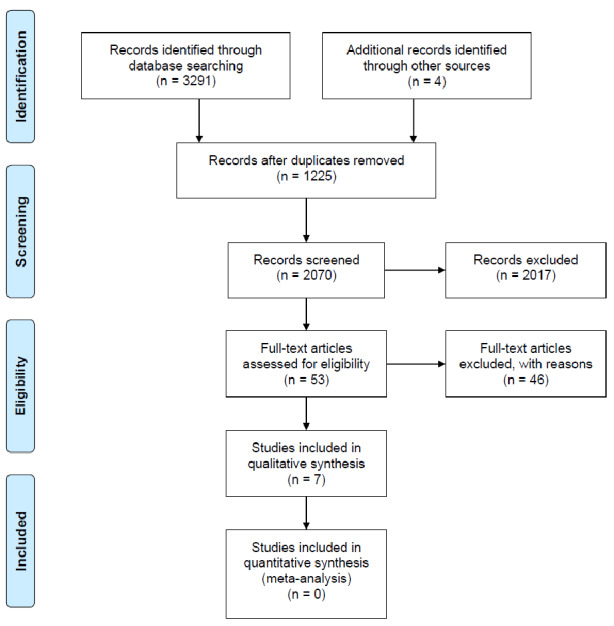
Methods: This systematic review included peer-reviewed journal articles. Searches of 7 databases and relevant reviews were conducted. Eligibility criteria consisted of studies that covered telemedicine as data- and information-sharing and two-way teleconsultation platforms, with the objective of supporting medical decisions (eg, diagnosis, treatment, and receiving hospital decision) in a prehospital emergency setting. Simulation studies and studies that included pediatric populations were excluded. The procedures in this review followed the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement. The Risk Of Bias In Non-randomised Studies-of Interventions (ROBINS-I) tool was used for the assessment of risk of bias. The results were synthesized based on predefined aspects of medical decisions that are made in a prehospital setting, which include diagnostic decision support, receiving facility decisions, and medical directions for treatment. All data extractions were done by at least two reviewers independently.
Results: Out of 42 full-text reviews, 7 were found eligible. Diagnostic support and medical direction and decision for treatments were often reported. A key finding of this review was the high agreement between prehospital diagnoses via telemedicine and final in-hospital diagnoses, as supported by quantitative evidence. However, a majority of the articles described the clinical value of having access to remote experts without robust quantitative data. Most telemedicine solutions were evaluated within a feasibility or short-term preliminary study. In general, the results were positive for telemedicine use; however, biases, due to preintervention confounding factors and a lack of documentation on quality assurance and protocol for telemedicine activation, make it difficult to determine the direct effect on patient outcomes.
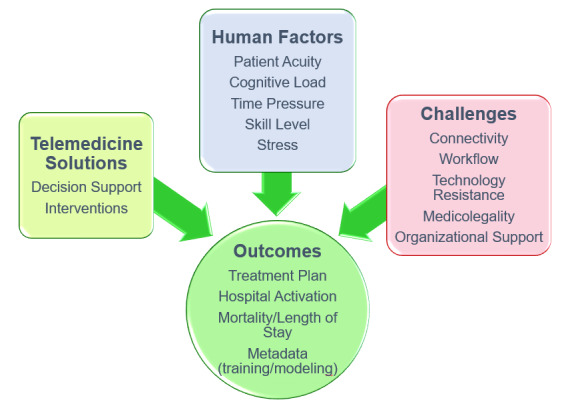
Conclusions: The information-sharing capacity of telemedicine enables access to remote experts to support medical decision making on scene or in prolonged field care. The influence of human and technology factors on patient care is poorly understood and documented.
Keywords: decision support; emergency; resuscitation; telemedicine.
©Yesul Kim, Christopher Groombridge, Lorena Romero, Steven Clare, Mark Christopher Fitzgerald. Originally published in the Journal of Medical Internet Research (http://www.jmir.org), 08.12.2020.
Conflict of interest statement
Conflicts of Interest: At the time of submission of this paper, the first author (YK) was the project manager for a project titled Ambulance Victoria HUD decision-support technology usability and effectiveness evaluation.
Figures
References
-
- Fitzgerald M, Reilly S, Smit DV, Kim Y, Mathew J, Boo E, Alqahtani A, Chowdhury S, Darez A, Mascarenhas JB, O'Keeffe F, Noonan M, Nickson C, Marquez M, Li WA, Zhang YL, Williams K, Mitra B. The World Health Organization trauma checklist versus Trauma Team Time-out: A perspective. Emerg Med Australas. 2019 Oct;31(5):882–885. doi: 10.1111/1742-6723.13306. http://europepmc.org/abstract/MED/31081585 - DOI - PMC - PubMed
-
- Valenzuela Espinoza A, De Smedt A, Guldolf K, Vandervorst F, Van Hooff R, Fernandez Tellez H, Desmaele S, Cambron M, Hubloue I, Brouns R. Opinions and beliefs about telemedicine for emergency treatment during ambulance transportation and for chronic care at home. Interact J Med Res. 2016 Mar 30;5(1):e9. doi: 10.2196/ijmr.5015. https://www.i-jmr.org/2016/1/e9/ - DOI - PMC - PubMed
-
- Terkelsen CJ, Nørgaard BL, Lassen JF, Gerdes JC, Ankersen JP, Rømer F, Nielsen TT, Andersen HR. Telemedicine used for remote prehospital diagnosing in patients suspected of acute myocardial infarction. J Intern Med. 2002 Nov;252(5):412–420. doi: 10.1046/j.1365-2796.2002.01051.x. https://onlinelibrary.wiley.com/resolve/openurl?genre=article&sid=nlm:pu... - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
