

Vitamin A levels reflect disease severity and portal hypertension in patients with cirrhosis
- PMID: 33289910
- PMCID: PMC7803875
- DOI: 10.1007/s12072-020-10112-3
Vitamin A levels reflect disease severity and portal hypertension in patients with cirrhosis
Abstract
Background and aims: The liver plays a key role in the storage, metabolism and homeostasis of fat-soluble vitamins. We investigated the relation of Vitamin(Vit)A/D/E serum levels with severity of liver disease and portal hypertension (PHT).
Methods: VitA/D/E serum levels were assessed in 234 patients with advanced chronic liver disease (ACLD, i.e. hepatic venous pressure gradient [HVPG] ≥ 6 mmHg). Patients with hepatocellular carcinoma, pre-/post-hepatic PHT, TIPS or liver transplantation were excluded.
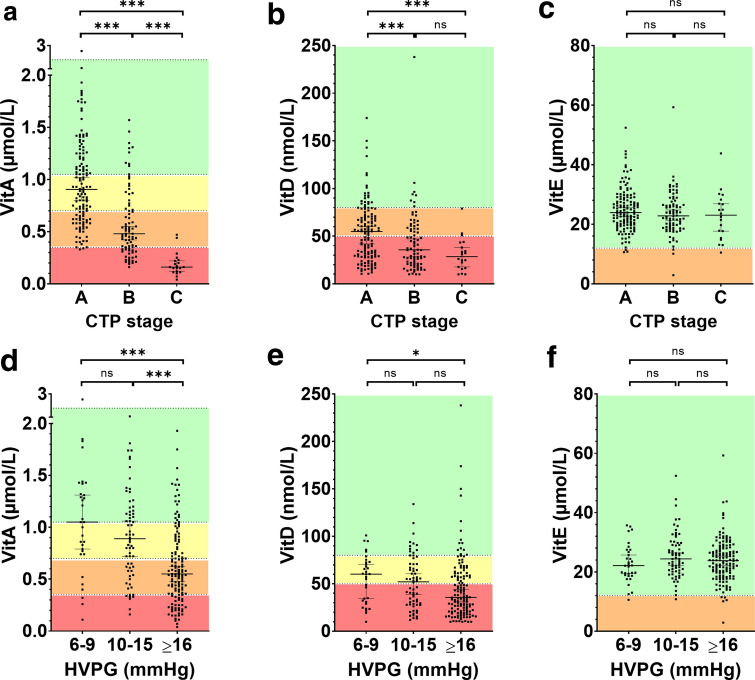
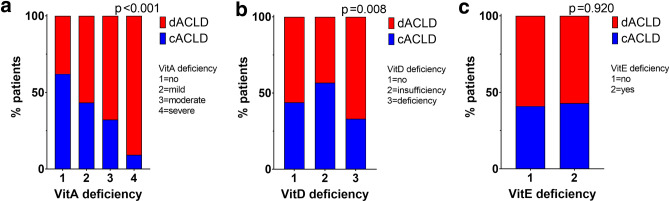
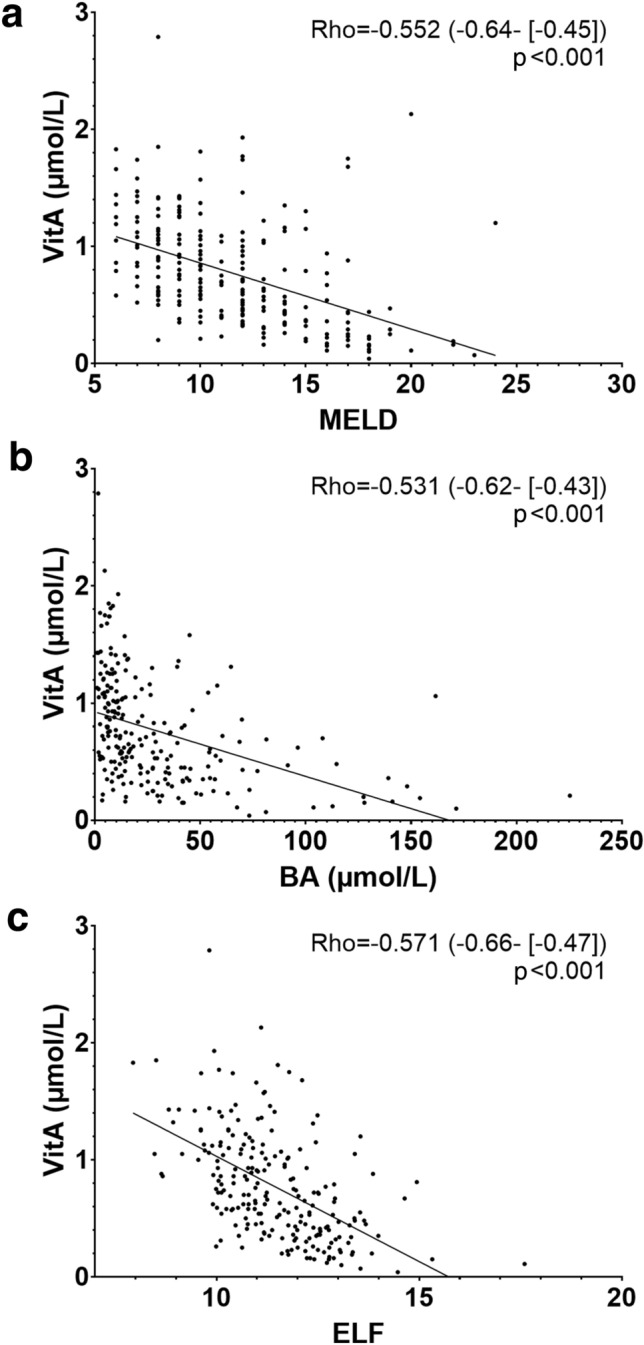
Results: Most patients were male (n = 153; 65%) with a median age of 57.6 (49.7-64.5) years. Thirty-two (14%) patients had HVPG 6-9 mmHg, 66 (28%) 10-15 mmHg, and 136 (58%) ≥ 16 mmHg, respectively. VitD deficiency (25-OH-vitamin-D <50 nmol/L) was found in 133 (57%) with higher prevalence in Child-Turcotte-Pugh (CTP)-C: 85% vs. B: 66% vs. A: 47% (p < 0.001). VitD levels displayed significant but weak correlations with hepatic dysfunction and PHT. VitE levels were normal in 227 (97%) patients and displayed no relevant association with hepatic dysfunction or PHT. Only 63 (27%) patients had normal (>1.05 µmol/L) VitA levels, while 58 (25%) had mild (0.70-1.04 µmol/L), 71 (30%) moderate (0.35-0.69 µmol/L), and 42(18%) severe(<0.35 µmol/L) VitA deficiency. VitA correlated with HVPG (Rho = -0.409), CTP score (Rho = -0.646), and serum bile acid levels (Rho = -0.531; all p < 0.001). The prevalence of decompensated ACLD (dACLD) continuously increased with severity of VitA deficiency (no: 40% vs. mild: 51% vs. moderate: 67% vs. severe: 91% had dACLD; p < 0.001). CTP score (per point; OR 2.46; 95%CI 1.80-3.37; p <0.001), age (per year; OR 0.95; 95%CI 0.92-0.98; p = 0.001) and elevated bile acid levels(>10 µmol/L; OR 3.62; 95%CI 1.61-8.14; p = 0.002) were independently associated with VitA deficiency.
Conclusion: VitA and VitD but not VitE deficiencies are highly prevalent in ACLD. VitA deficiency strongly correlates with hepatic dysfunction, PHT and bile acid levels and is associated with decompensated ACLD.
Trial registration number: NCT03267615.
Keywords: ACLD; Cirrhosis; Hepatic decompensation; Hepatic venous pressure gradient.
Conflict of interest statement
BeSi received travel support from AbbVie and Gilead. BeSc received travel support from Abbvie and Gilead. PS received speaking honoraria from Bristol-Myers Squibb and Boehringer-Ingelheim, consulting fees from PharmaIN, and travel support from Falk and Phenex Pharmaceuticals. DB received travel support from AbbVie and Gilead. TB received speaker honoraria from BMS, travel support from Abbvie, BMS, and Gilead; travel grant, financial award/grant from Medis. MP is an investigator for Bayer, BMS, Lilly, and Roche; he received speaker honoraria from Bayer, BMS, Eisai, and MSD; he is a consultant for Bayer, BMS, Ipsen, Eisai, Lilly, MSD, and Roche; he received travel support from Bayer and BMS. MT received speaker fees from BMS, Falk Foundation, Gilead, Intercept and MSD; advisory board fees from Albireo, BiomX, Boehringer Ingelheim, Falk Pharma GmbH, Genfit, Gilead, Intercept, MSD, Novartis, Phenex and Regulus. He further received travel grants from Abbvie, Falk, Gilead and Intercept and unrestricted research grants from Albireo, Cymabay, Falk, Gilead, Intercept, MSD and Takeda. MM has served as a speaker and/or consultant and/or advisory board member for AbbVie, Bristol-Myers Squibb, Gilead, W.L. Gore & Associates and Janssen. TR received grant support from Abbvie, Boehringer-Ingelheim, Gilead, MSD, Philips Healthcare, Gore; speaking honoraria from Abbvie, Gilead, Gore, Intercept, Roche, MSD; consulting/advisory board fee from Abbvie, Bayer, Boehringer-Ingelheim, Gilead, MSD, Siemens; and travel support from Boehringer-Ingelheim, Gilead and Roche. GS, AFS, AS, EE, and RP declare no conflict of interest.
Figures
References
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
