

RV144 HIV-1 vaccination impacts post-infection antibody responses
- PMID: 33290394
- PMCID: PMC7748270
- DOI: 10.1371/journal.ppat.1009101
RV144 HIV-1 vaccination impacts post-infection antibody responses
Erratum in
-
Correction: RV144 HIV-1 vaccination impacts post-infection antibody responses.PLoS Pathog. 2021 Mar 2;17(3):e1009386. doi: 10.1371/journal.ppat.1009386. eCollection 2021 Mar. PLoS Pathog. 2021. PMID: 33651828 Free PMC article.
Abstract
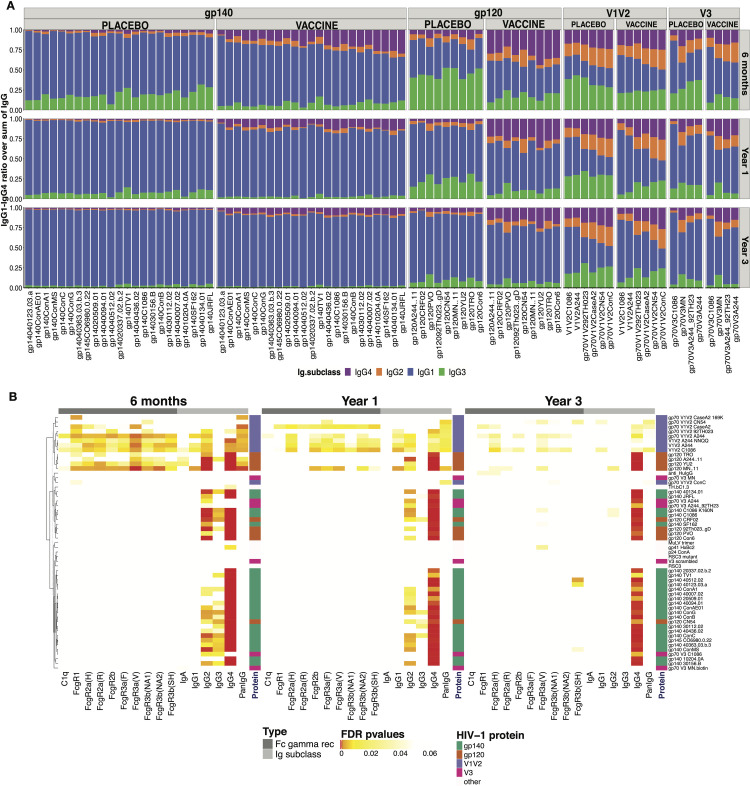
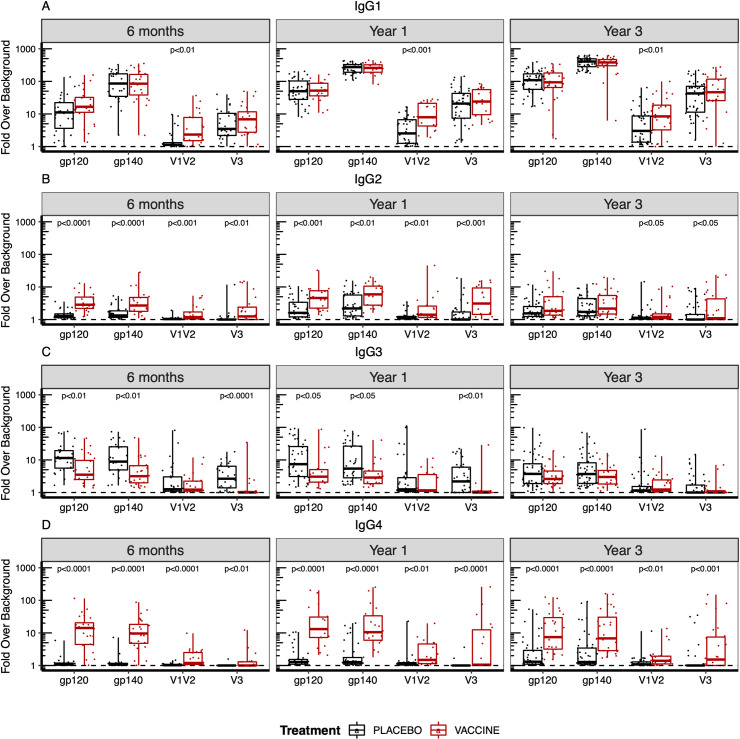
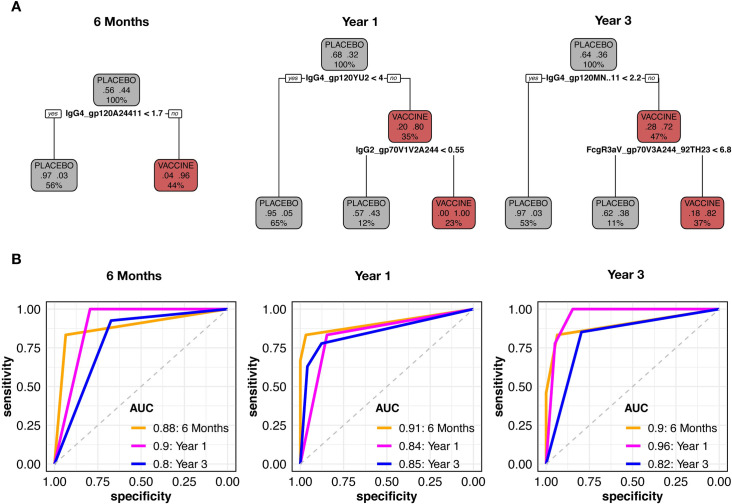
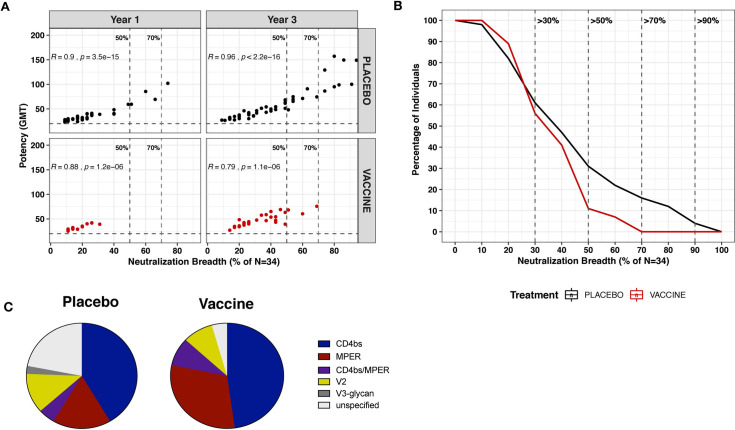
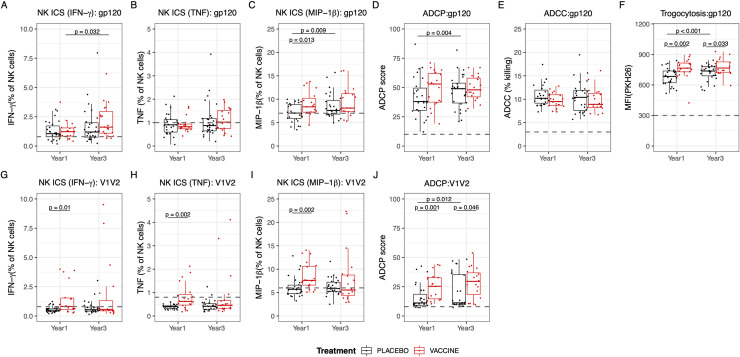
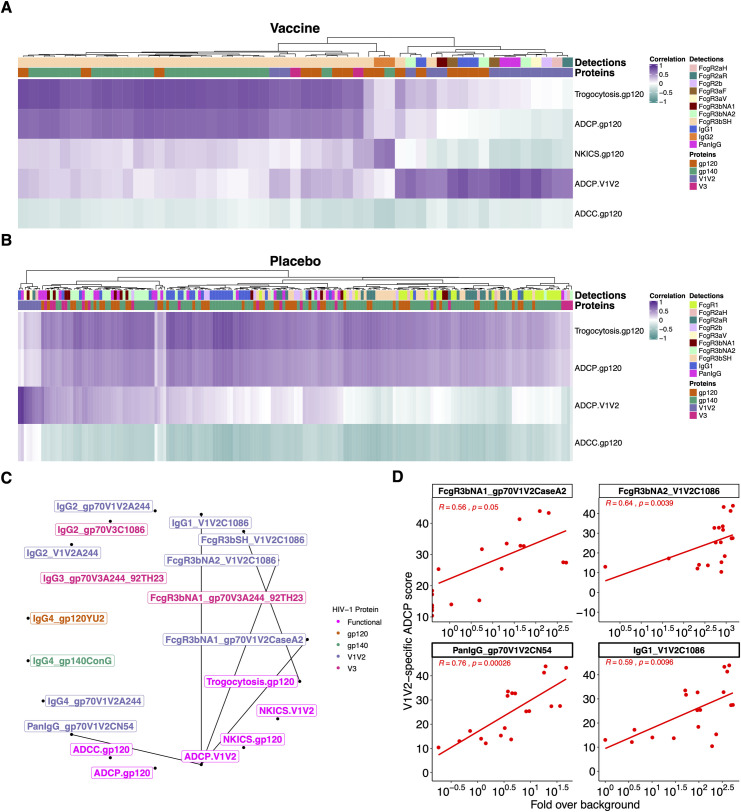
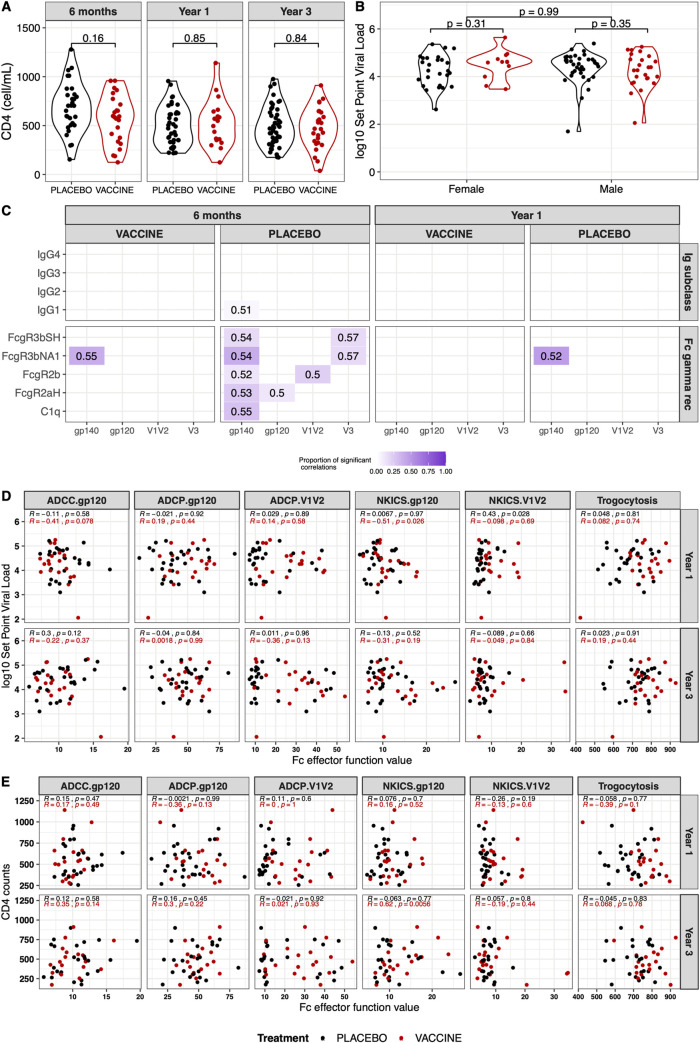
The RV144 vaccine efficacy clinical trial showed a reduction in HIV-1 infections by 31%. Vaccine efficacy was associated with stronger binding antibody responses to the HIV Envelope (Env) V1V2 region, with decreased efficacy as responses wane. High levels of Ab-dependent cellular cytotoxicity (ADCC) together with low plasma levels of Env-specific IgA also correlated with decreased infection risk. We investigated whether B cell priming from RV144 vaccination impacted functional antibody responses to HIV-1 following infection. Antibody responses were assessed in 37 vaccine and 63 placebo recipients at 6, 12, and 36 months following HIV diagnosis. The magnitude, specificity, dynamics, subclass recognition and distribution of the binding antibody response following infection were different in RV144 vaccine recipients compared to placebo recipients. Vaccine recipients demonstrated increased IgG1 binding specifically to V1V2, as well as increased IgG2 and IgG4 but decreased IgG3 to HIV-1 Env. No difference in IgA binding to HIV-1 Env was detected between the vaccine and placebo recipients following infection. RV144 vaccination limited the development of broadly neutralizing antibodies post-infection, but enhanced Fc-mediated effector functions indicating B cell priming by RV144 vaccination impacted downstream antibody function. However, these functional responses were not associated with clinical markers of disease progression. These data reveal that RV144 vaccination primed B cells towards specific binding and functional antibody responses following HIV-1 infection.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
