

Induction of labour at 41 weeks or expectant management until 42 weeks: A systematic review and an individual participant data meta-analysis of randomised trials
- PMID: 33290410
- PMCID: PMC7723286
- DOI: 10.1371/journal.pmed.1003436
Induction of labour at 41 weeks or expectant management until 42 weeks: A systematic review and an individual participant data meta-analysis of randomised trials
Abstract
Background: The risk of perinatal death and severe neonatal morbidity increases gradually after 41 weeks of pregnancy. Several randomised controlled trials (RCTs) have assessed if induction of labour (IOL) in uncomplicated pregnancies at 41 weeks will improve perinatal outcomes. We performed an individual participant data meta-analysis (IPD-MA) on this subject.
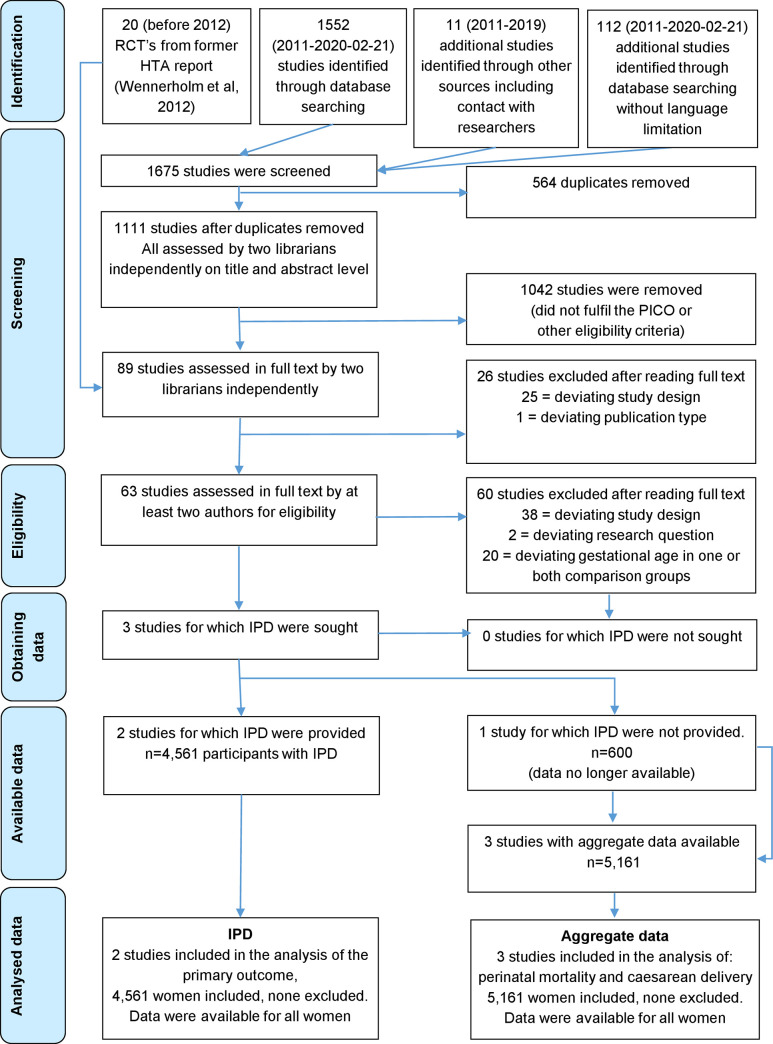
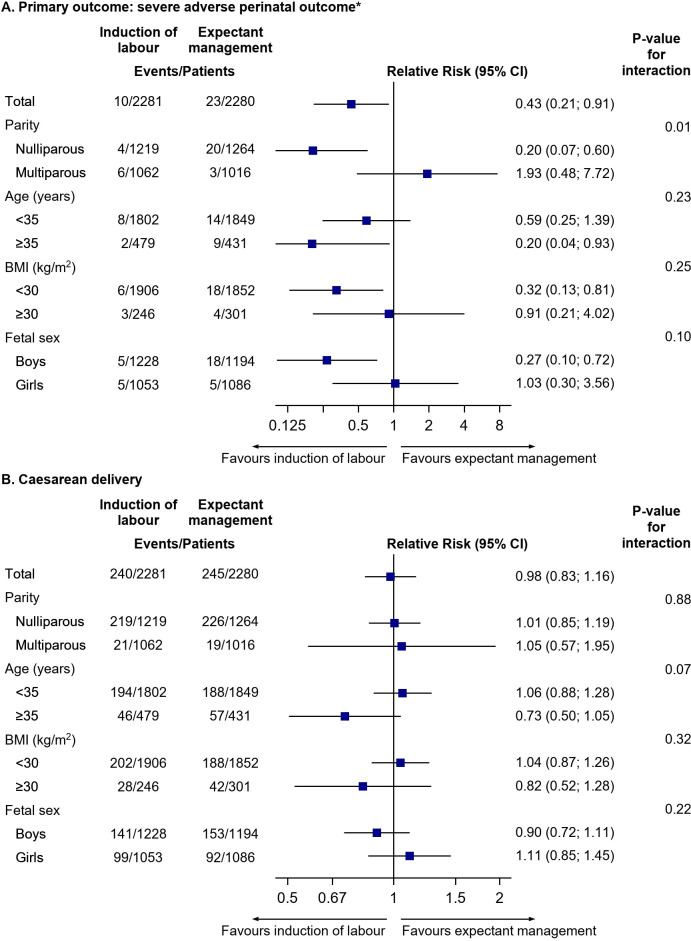
Methods and findings: We searched PubMed, Excerpta Medica dataBASE (Embase), The Cochrane Library, Cumulative Index of Nursing and Allied Health Literature (CINAHL), and PsycINFO on February 21, 2020 for RCTs comparing IOL at 41 weeks with expectant management until 42 weeks in women with uncomplicated pregnancies. Individual participant data (IPD) were sought from eligible RCTs. Primary outcome was a composite of severe adverse perinatal outcomes: mortality and severe neonatal morbidity. Additional outcomes included neonatal admission, mode of delivery, perineal lacerations, and postpartum haemorrhage. Prespecified subgroup analyses were conducted for parity (nulliparous/multiparous), maternal age (<35/≥35 years), and body mass index (BMI) (<30/≥30). Aggregate data meta-analysis (MA) was performed to include data from RCTs for which IPD was not available. From 89 full-text articles, we identified three eligible RCTs (n = 5,161), and two contributed with IPD (n = 4,561). Baseline characteristics were similar between the groups regarding age, parity, BMI, and higher level of education. IOL resulted overall in a decrease of severe adverse perinatal outcome (0.4% [10/2,281] versus 1.0% [23/2,280]; relative risk [RR] 0.43 [95% confidence interval [CI] 0.21 to 0.91], p-value 0.027, risk difference [RD] -57/10,000 [95% CI -106/10,000 to -8/10,000], I2 0%). The number needed to treat (NNT) was 175 (95% CI 94 to 1,267). Perinatal deaths occurred in one (<0.1%) versus eight (0.4%) pregnancies (Peto odds ratio [OR] 0.21 [95% CI 0.06 to 0.78], p-value 0.019, RD -31/10,000, [95% CI -56/10,000 to -5/10,000], I2 0%, NNT 326, [95% CI 177 to 2,014]) and admission to a neonatal care unit ≥4 days occurred in 1.1% (24/2,280) versus 1.9% (46/2,273), (RR 0.52 [95% CI 0.32 to 0.85], p-value 0.009, RD -97/10,000 [95% CI -169/10,000 to -26/10,000], I2 0%, NNT 103 [95% CI 59 to 385]). There was no difference in the rate of cesarean delivery (10.5% versus 10.7%; RR 0.98, [95% CI 0.83 to 1.16], p-value 0.81) nor in other important perinatal, delivery, and maternal outcomes. MA on aggregate data showed similar results. Prespecified subgroup analyses for the primary outcome showed a significant difference in the treatment effect (p = 0.01 for interaction) for parity, but not for maternal age or BMI. The risk of severe adverse perinatal outcome was decreased for nulliparous women in the IOL group (0.3% [4/1,219] versus 1.6% [20/1,264]; RR 0.20 [95% CI 0.07 to 0.60], p-value 0.004, RD -127/10,000, [95% CI -204/10,000 to -50/10,000], I2 0%, NNT 79 [95% CI 49 to 201]) but not for multiparous women (0.6% [6/1,219] versus 0.3% [3/1,264]; RR 1.59 [95% CI 0.15 to 17.30], p-value 0.35, RD 27/10,000, [95% CI -29/10,000 to 84/10,000], I2 55%). A limitation of this IPD-MA was the risk of overestimation of the effect on perinatal mortality due to early stopping of the largest included trial for safety reasons after the advice of the Data and Safety Monitoring Board. Furthermore, only two RCTs were eligible for the IPD-MA; thus, the possibility to assess severe adverse neonatal outcomes with few events was limited.
Conclusions: In this study, we found that, overall, IOL at 41 weeks improved perinatal outcome compared with expectant management until 42 weeks without increasing the cesarean delivery rate. This benefit is shown only in nulliparous women, whereas for multiparous women, the incidence of mortality and morbidity was too low to demonstrate any effect. The magnitude of risk reduction of perinatal mortality remains uncertain. Women with pregnancies approaching 41 weeks should be informed on the risk differences according to parity so that they are able to make an informed choice for IOL at 41 weeks or expectant management until 42 weeks. Study Registration: PROSPERO CRD42020163174.
Conflict of interest statement
I have read the journal's policy and the authors of this manuscript have the following competing interests: BWM is supported by a NHMRC Practitioner Fellowship (GNT1082548) BWM reports consultancy for ObsEva, Merck Merck KGaA and Guerbet
Figures
Similar articles
-
Induction of labour at or beyond 37 weeks' gestation.Cochrane Database Syst Rev. 2020 Jul 15;7(7):CD004945. doi: 10.1002/14651858.CD004945.pub5. Cochrane Database Syst Rev. 2020. PMID: 32666584 Free PMC article.
-
Induction of labour at 41 weeks versus expectant management until 42 weeks (INDEX): multicentre, randomised non-inferiority trial.BMJ. 2019 Feb 20;364:l344. doi: 10.1136/bmj.l344. BMJ. 2019. PMID: 30786997 Free PMC article. Clinical Trial.
-
Induction of labour at 39 weeks and adverse outcomes in low-risk pregnancies according to ethnicity, socioeconomic deprivation, and parity: A national cohort study in England.PLoS Med. 2023 Jul 20;20(7):e1004259. doi: 10.1371/journal.pmed.1004259. eCollection 2023 Jul. PLoS Med. 2023. PMID: 37471395 Free PMC article.
-
Induction of labour at 41 weeks versus expectant management and induction of labour at 42 weeks (SWEdish Post-term Induction Study, SWEPIS): multicentre, open label, randomised, superiority trial.BMJ. 2019 Nov 20;367:l6131. doi: 10.1136/bmj.l6131. BMJ. 2019. PMID: 31748223 Free PMC article. Clinical Trial.
-
Elective induction of labor at 39 weeks compared with expectant management: a meta-analysis of cohort studies.Am J Obstet Gynecol. 2019 Oct;221(4):304-310. doi: 10.1016/j.ajog.2019.02.046. Epub 2019 Feb 25. Am J Obstet Gynecol. 2019. PMID: 30817905
Cited by
-
Labor induction at 41+0 gestational weeks or expectant management for the nulliparous woman: The Finnish randomized controlled multicenter trial.Acta Obstet Gynecol Scand. 2024 Mar;103(3):505-511. doi: 10.1111/aogs.14755. Epub 2023 Dec 19. Acta Obstet Gynecol Scand. 2024. PMID: 38112629 Free PMC article. Clinical Trial.
-
Perinatal mortality and neonatal and maternal outcome per gestational week in term pregnancies: A registry-based study.Acta Obstet Gynecol Scand. 2023 Jan;102(1):82-91. doi: 10.1111/aogs.14467. Epub 2022 Oct 20. Acta Obstet Gynecol Scand. 2023. PMID: 36263854 Free PMC article.
-
Association between miRNAs in serum at 10-14 gestational weeks and spontaneous preterm delivery.Acta Obstet Gynecol Scand. 2024 Oct;103(10):2013-2023. doi: 10.1111/aogs.14926. Epub 2024 Jul 21. Acta Obstet Gynecol Scand. 2024. PMID: 39034527 Free PMC article.
-
Time of delivery among low-risk women at 37-42 weeks of gestation and risks of stillbirth and infant mortality, and long-term neurological morbidity.Paediatr Perinat Epidemiol. 2022 Jul;36(4):577-587. doi: 10.1111/ppe.12868. Epub 2022 Mar 4. Paediatr Perinat Epidemiol. 2022. PMID: 35244233 Free PMC article.
-
Does induction of labor at 41 weeks (early, mid or late) improve birth outcomes in low-risk pregnancy? A nationwide propensity score-matched study.Acta Obstet Gynecol Scand. 2023 May;102(5):612-625. doi: 10.1111/aogs.14536. Epub 2023 Mar 13. Acta Obstet Gynecol Scand. 2023. PMID: 36915238 Free PMC article.
References
-
- Muglu J, Rather H, Arroyo-Manzano D, Bhattacharya S, Balchin I, Khalil A, et al. Risks of stillbirth and neonatal death with advancing gestation at term: A systematic review and meta-analysis of cohort studies of 15 million pregnancies. PLoS Med. 2019;16(7):e1002838 Epub 2019 Jul 3. 10.1371/journal.pmed.1002838 - DOI - PMC - PubMed
-
- Linder N, Hiersch L, Fridman E, Klinger G, Lubin D, Kouadio F, et al. Post-term pregnancy is an independent risk factor for neonatal morbidity even in low-risk singleton pregnancies. Arch Dis Child Fetal Neonatal Ed. 2017;102(4):F286–90. Epub 2015 Dec 10. 10.1136/archdischild-2015-308553 . - DOI - PubMed
-
- Seijmonsbergen-Schermers AE, van den Akker T, Rydahl E, Beeckman K, Bogaerts A, Binfa L, et al. Variations in use of childbirth interventions in 13 high-income countries: A multinational cross-sectional study. PLoS Med. 2020;17(5):e1003103 Epub 2020 May 23. 10.1371/journal.pmed.1003103 - DOI - PMC - PubMed
-
- The Swedish Pregnancy Register. Available from: https://www.medscinet.com/GR/english.aspx.
-
- Perined. Perinatale zorg in Nederland anno 2018: landelijke perinatale cijfers en duiding. Utrecht 2019.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
