

Assessing clinical quality performance and staffing capacity differences between urban and rural Health Resources and Services Administration-funded health centers in the United States: A cross sectional study
- PMID: 33290435
- PMCID: PMC7723285
- DOI: 10.1371/journal.pone.0242844
Assessing clinical quality performance and staffing capacity differences between urban and rural Health Resources and Services Administration-funded health centers in the United States: A cross sectional study
Abstract
Background: In the United States, there are nearly 1,400 Health Resources and Services Administration-funded health centers (HCs) serving low-income and underserved populations and more than 600 of these HCs are located in rural areas. Disparities in quality of medical care in urban vs. rural areas exist but data on such differences between urban and rural HCs is limited in the literature. We examined whether urban and rural HCs differed in their performance on clinical quality measures before and after controlling for patient, organizational, and contextual characteristics.
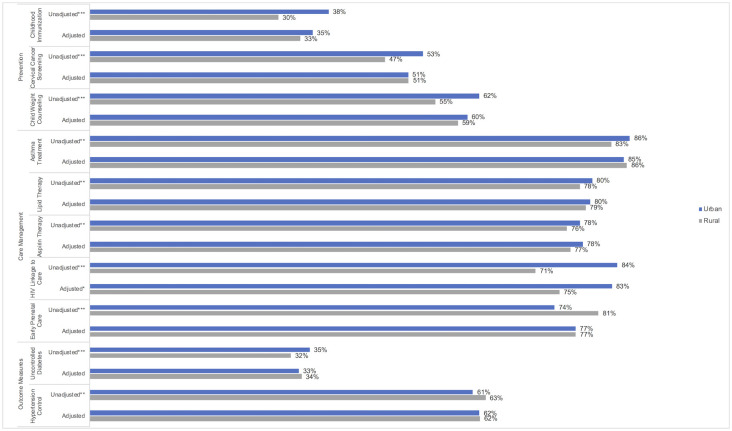
Methods and findings: We used the 2017 Uniform Data System to examine performance on clinical quality measures between urban and rural HCs (n = 1,373). We used generalized linear regression models with the logit link function and binomial distribution, controlling for confounding factors. After adjusting for potential confounders, we found on par performance between urban and rural HCs in all but one clinical quality measure. Rural HCs had lower rates of linking patients newly diagnosed with HIV to care (74% [95% CI: 69%, 80%] vs. 83% [95% CI: 80%, 86%]). We identified control variables that systematically accounted for eliminating urban vs. rural differences in performance on clinical quality measures. We also found that both urban and rural HCs had some clinical quality performance measures that were lower than available national benchmarks. Main limitations included potential discrepancy of urban or rural designation across all HC sites within a HC organization.
Conclusions: Findings highlight HCs' contributions in addressing rural disparities in quality of care and identify opportunities for improvement. Performance in both rural and urban HCs may be improved by supporting programs that increase the availability of providers, training, and provision of technical resources.
Conflict of interest statement
The authors have read the journal’s policy, and the authors of this manuscript have the following competing interests to declare: HH and AS are employees of the U.S. Government, U.S. Department of Health and Human Services, which funded this study. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
References
-
- U.S. Department of Agriculture Economic Research Service. Population and Migration, Overview 2017 [cited 2017 8/21]. https://www.ers.usda.gov/topics/rural-economy-population/population-migr....
-
- Agency for Healthcare Research and Quality. National Healthcare Quality and Disparities Report chartbook on rural health care. Rockville, MD: October 2017. - PubMed
-
- North Carolina Rural Health Research Program. Rural Health Snapshot (2017). Cecil G. Sheps Center for Health Services Research, The University of North Carolina at Chapel Hill, 2017.
-
- Larson SL, Fleishman JA. Rural-Urban Differences in Usual Source of Care and Ambulatory Service Use: Analyses of National Data Using Urban Influence Codes. Medical Care. 2003;41(7):III-65–III-74. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
