

Responsiveness to Parenteral Corticosteroids and Lung Function Trajectory in Adults with Moderate-to-Severe Asthma
- PMID: 33290668
- PMCID: PMC8017577
- DOI: 10.1164/rccm.202002-0454OC
Responsiveness to Parenteral Corticosteroids and Lung Function Trajectory in Adults with Moderate-to-Severe Asthma
Abstract
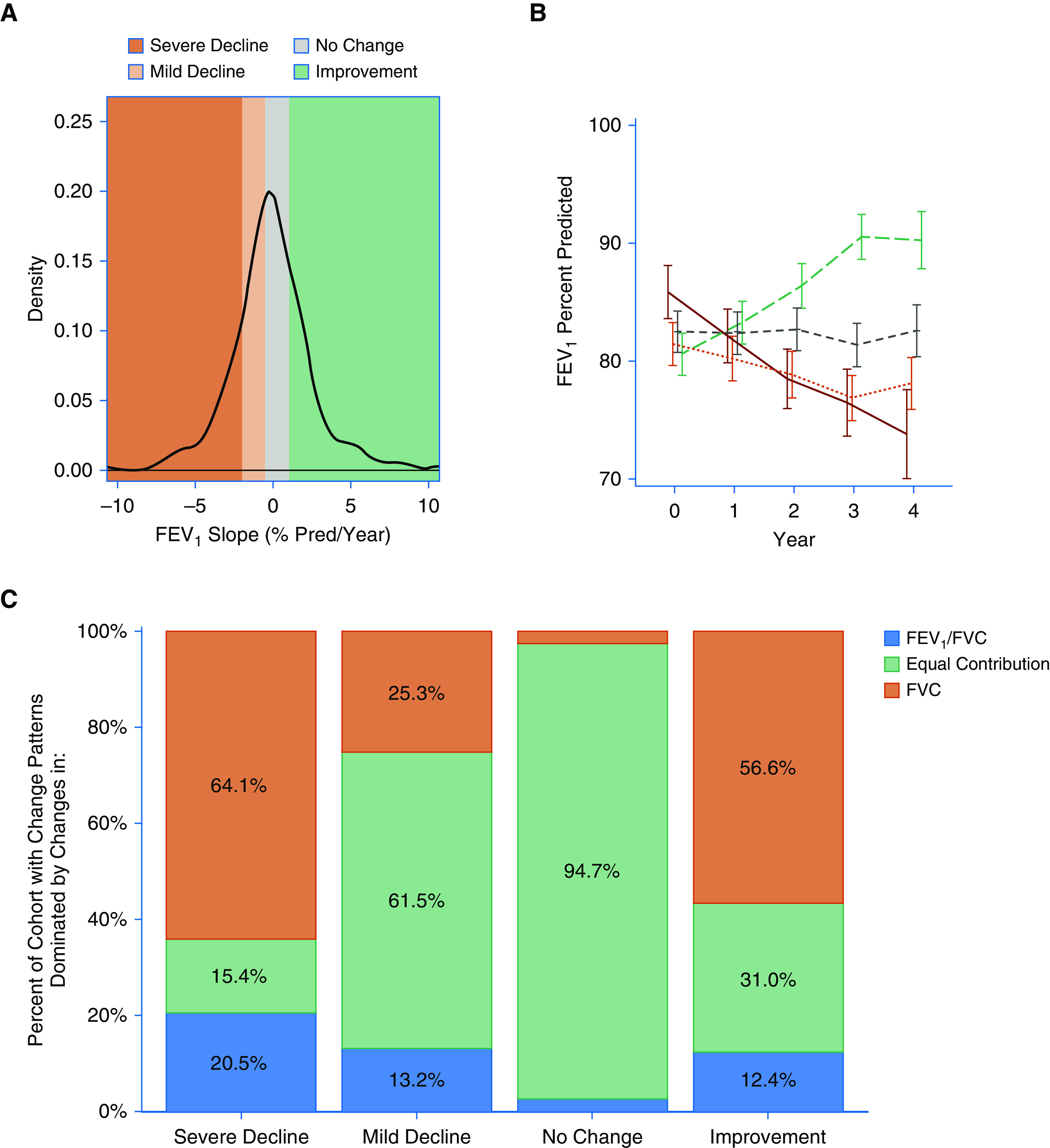
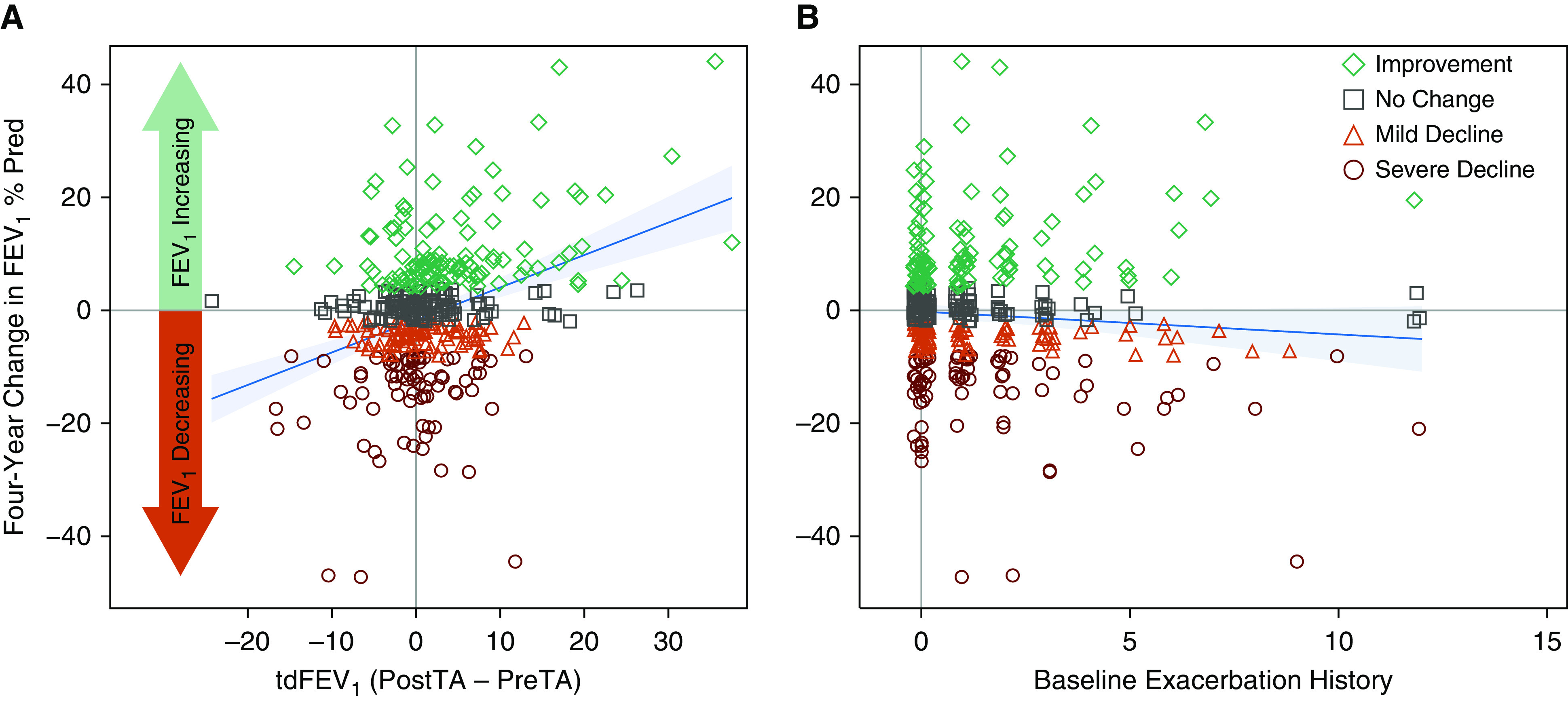
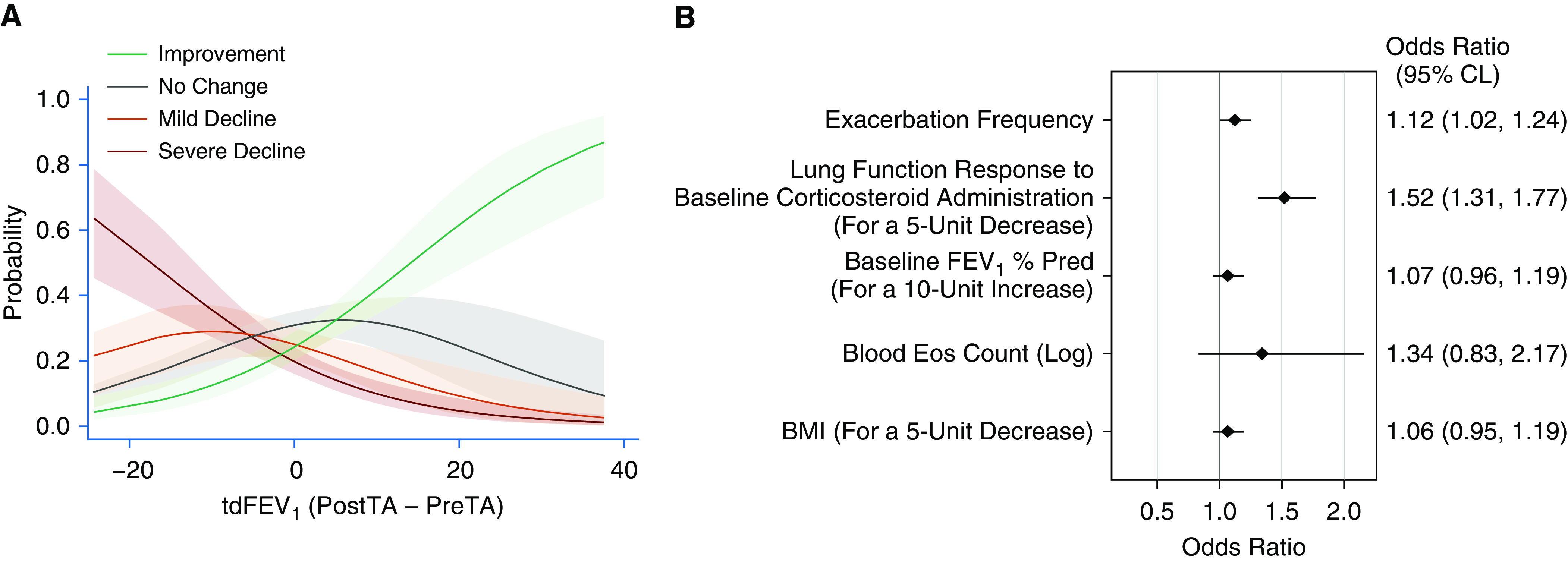
Rationale: It is unclear why select patients with moderate-to-severe asthma continue to lose lung function despite therapy. We hypothesized that participants with the smallest responses to parenteral corticosteroids have the greatest risk of undergoing a severe decline in lung function.Objectives: To evaluate corticosteroid-response phenotypes as longitudinal predictors of lung decline.Methods: Adults within the NHLBI SARP III (Severe Asthma Research Program III) who had undergone a course of intramuscular triamcinolone at baseline and at ≥2 annual follow-up visits were evaluated. Longitudinal slopes were calculated for each participant's post-bronchodilator FEV1% predicted. Categories of participant FEV1 slope were defined: severe decline, >2% loss/yr; mild decline, >0.5-2.0% loss/yr; no change, 0.5% loss/yr to <1% gain/yr; and improvement, ≥1% gain/yr. Regression models were used to develop predictors of severe decline.Measurements and Main Results: Of 396 participants, 78 had severe decline, 91 had mild decline, 114 had no change, and 113 showed improvement. The triamcinolone-induced difference in the post-bronchodilator FEV1% predicted (derived by baseline subtraction) was related to the 4-year change in lung function or slope category in univariable models (P < 0.001). For each 5% decrement in the triamcinolone-induced difference the FEV1% predicted, there was a 50% increase in the odds of being in the severe decline group (odds ratio, 1.5; 95% confidence interval, 1.3-1.8), when adjusted for baseline FEV1, exacerbation history, blood eosinophils and body mass index.Conclusions: Failure to improve the post-bronchodilator FEV1 after a challenge with parenteral corticosteroids is an evoked biomarker for patients at risk for a severe decline in lung function.
Keywords: corticosteroid sensitivity; exacerbations; longitudinal; lung function; severe asthma.
Figures

Comment in
-
Response to Parenteral Triamcinolone in Severe Asthma: A Useful Induced Phenotype for Clinicians?Am J Respir Crit Care Med. 2021 Apr 1;203(7):790-791. doi: 10.1164/rccm.202012-4485ED. Am J Respir Crit Care Med. 2021. PMID: 33449842 Free PMC article. No abstract available.
References
-
- Peat JK, Woolcock AJ, Cullen K. Rate of decline of lung function in subjects with asthma. Eur J Respir Dis. 1987;70:171–179. - PubMed
-
- Van Schayck CP, Dompeling E, Van Herwaarden CL, Wever AM, Van Weel C. Interacting effects of atopy and bronchial hyperresponsiveness on the annual decline in lung function and the exacerbation rate in asthma. Am Rev Respir Dis. 1991;144:1297–1301. - PubMed
-
- Haahtela T, Järvinen M, Kava T, Kiviranta K, Koskinen S, Lehtonen K, et al. Comparison of a beta 2-agonist, terbutaline, with an inhaled corticosteroid, budesonide, in newly detected asthma. N Engl J Med. 1991;325:388–392. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- U10 HL109257/HL/NHLBI NIH HHS/United States
- UL1 TR000427/TR/NCATS NIH HHS/United States
- K23 AI125785/AI/NIAID NIH HHS/United States
- U01 HL146002/HL/NHLBI NIH HHS/United States
- U10 HL109250/HL/NHLBI NIH HHS/United States
- UG1 HL139126/HL/NHLBI NIH HHS/United States
- U10 HL109164/HL/NHLBI NIH HHS/United States
- U10 HL109172/HL/NHLBI NIH HHS/United States
- UL1 TR000454/TR/NCATS NIH HHS/United States
- UL1 TR001420/TR/NCATS NIH HHS/United States
- UL1 TR002373/TR/NCATS NIH HHS/United States
- U10 HL109086/HL/NHLBI NIH HHS/United States
- U10 HL109168/HL/NHLBI NIH HHS/United States
- UL1 TR001102/TR/NCATS NIH HHS/United States
- UL1 TR002366/TR/NCATS NIH HHS/United States
- U10 HL109152/HL/NHLBI NIH HHS/United States
- U10 HL109146/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
