

Diagnosis and Management of Acute Respiratory Distress Syndrome in a Time of COVID-19
- PMID: 33291238
- PMCID: PMC7762111
- DOI: 10.3390/diagnostics10121053
Diagnosis and Management of Acute Respiratory Distress Syndrome in a Time of COVID-19
Abstract
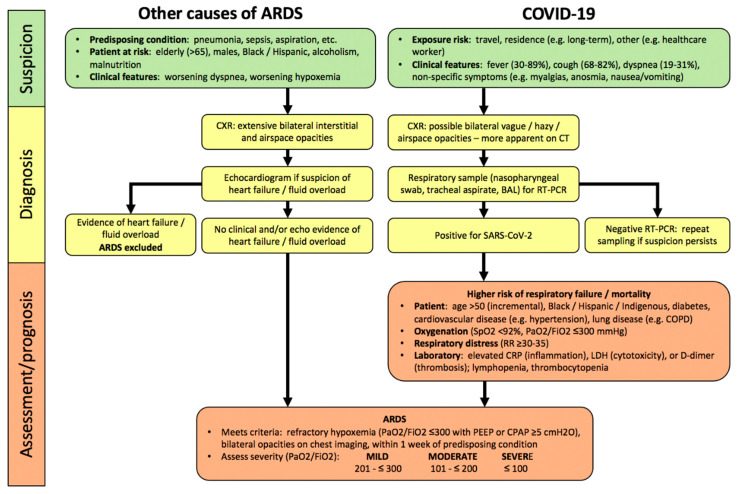
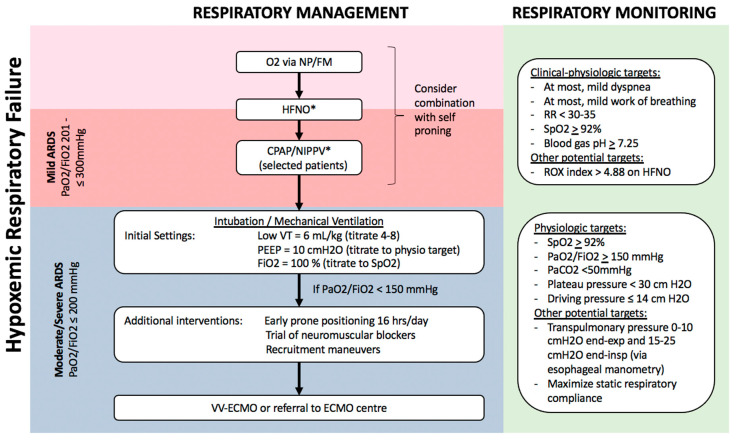
Acute respiratory distress syndrome (ARDS) remains a serious illness with significant morbidity and mortality, characterized by hypoxemic respiratory failure most commonly due to pneumonia, sepsis, and aspiration. Early and accurate diagnosis of ARDS depends upon clinical suspicion and chest imaging. Coronavirus disease 2019 (COVID-19) is an important novel cause of ARDS with a distinct time course, imaging and laboratory features from the time of SARS-CoV-2 infection to hypoxemic respiratory failure, which may allow diagnosis and management prior to or at earlier stages of ARDS. Treatment of ARDS remains largely supportive, and consists of incremental respiratory support (high flow nasal oxygen, non-invasive respiratory support, and invasive mechanical ventilation), and avoidance of iatrogenic complications, all of which improve clinical outcomes. COVID-19-associated ARDS is largely similar to other causes of ARDS with respect to pathology and respiratory physiology, and as such, COVID-19 patients with hypoxemic respiratory failure should typically be managed as other patients with ARDS. Non-invasive respiratory support may be beneficial in avoiding intubation in COVID-19 respiratory failure including mild ARDS, especially under conditions of resource constraints or to avoid overwhelming critical care resources. Compared to other causes of ARDS, medical therapies may improve outcomes in COVID-19-associated ARDS, such as dexamethasone and remdesivir. Future improved clinical outcomes in ARDS of all causes depends upon individual patient physiological and biological endotyping in order to improve accuracy and timeliness of diagnosis as well as optimal targeting of future therapies in the right patient at the right time in their disease.
Keywords: COVID-19; SARS-CoV-2; acute respiratory distress syndrome (ARDS); dexamethasone; high flow nasal oxygen; mechanical ventilation; non-invasive ventilation.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Ranieri V.M., Rubenfeld G.D., Thompson B.T., Ferguson N.D., Caldwell E., Fan E. Acute respiratory distress syndrome: The Berlin Definition. JAMA. 2012;307:2526–2533. - PubMed
-
- Bellani G., Laffey J.G., Pham T., Fan E., Brochard L., Esteban A., Gattinoni L., Van Haren F., Larsson A., McAuley D.F., et al. Epidemiology, Patterns of Care, and Mortality for Patients with Acute Respiratory Distress Syndrome in Intensive Care Units in 50 Countries. JAMA. 2016;315:788–800. doi: 10.1001/jama.2016.0291. - DOI - PubMed
-
- Brun-Buisson C., Minelli C., Bertolini G., Brazzi L., Pimentel J., Lewandowski K., Bion J., Romand J.-A., Villar J., Thorsteinsson A., et al. Epidemiology and outcome of acute lung injury in European intensive care units. Intensive Care Med. 2004;30:51–61. doi: 10.1007/s00134-003-2022-6. - DOI - PubMed
-
- Cheung A., Tansey C.M., Tomlinson G., Diaz-Granados N., Matte A., Barr A., Mehta S., Mazer C.D., Guest C.B., Stewart T.E., et al. Two-Year Outcomes, Health Care Use, and Costs of Survivors of Acute Respiratory Distress Syndrome. Am. J. Respir. Crit. Care Med. 2006;174:538–544. doi: 10.1164/rccm.200505-693OC. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
