

Investigating the Psychological Impact of COVID-19 among Healthcare Workers: A Meta-Analysis
- PMID: 33291511
- PMCID: PMC7730003
- DOI: 10.3390/ijerph17239096
Investigating the Psychological Impact of COVID-19 among Healthcare Workers: A Meta-Analysis
Abstract
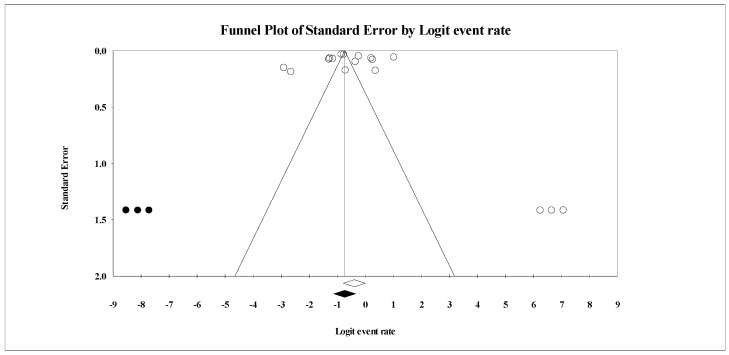
Previous meta-analyses were conducted during the initial phases of the COVID-19 pandemic, which utilized a smaller pool of data. The current meta-analysis aims to provide additional (and updated) evidence related to the psychological impact among healthcare workers. The search strategy was developed by a medical librarian and bibliographical databases, including Medline, Embase, CINAHL, PsycINFO, and Scopus were searched for studies examining the impact of the COVID-19 pandemic on the psychological health of healthcare workers. Articles were screened by three reviewers. Heterogeneity among studies was assessed by I2 statistic. The random-effects model was utilized to obtain the pooled prevalence. A subgroup analysis by region, gender, quality of study, assessment methods, healthcare profession, and exposure was performed. Publication bias was assessed by Funnel plot and Egger linear regression test. Sixty-five studies met the inclusion criteria and the total sample constituted 79,437 participants. The pooled prevalence of anxiety, depression, stress, post-traumatic stress syndrome, insomnia, psychological distress, and burnout was 34.4%, 31.8%, 40.3%, 11.4%, 27.8%, 46.1%, and 37.4% respectively. The subgroup analysis indicated higher anxiety and depression prevalence among females, nurses, and frontline responders than males, doctors, and second-line healthcare workers. This study highlights the need for designing a targeted intervention to improve resilience and foster post-traumatic growth among frontline responders.
Keywords: COVID-19; SARS-COV-2; anxiety; burnout; depression; fatigue; insomnia; post-traumatic stress syndrome; psychological; stress.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
















References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
