

Improving agreement of ASA physical status class between pre-anesthesia screening and day of surgery by adding institutional-specific and ASA-approved examples: a quality improvement project
- PMID: 33292640
- PMCID: PMC7677831
- DOI: 10.1186/s13741-020-00162-4
Improving agreement of ASA physical status class between pre-anesthesia screening and day of surgery by adding institutional-specific and ASA-approved examples: a quality improvement project
Abstract
Background: A successful anesthesia pre-assessment clinic needs to identify patients who need further testing, evaluation, and optimization prior to the day of surgery to avoid delays and cancelations. Although the ASA Physical Status Classification system (ASA PS) has been used widely for over 50 years, it has poor interrater agreement when only using the definitions. In 2014, ASA-approved examples for each ASA physical status class (ASA PS). In this quality improvement study, we developed and evaluated the effectiveness of institutional-specific examples on interrater reliability between anesthesia pre-anesthesia clinic (APAC) and the day of surgery evaluation (DOS).
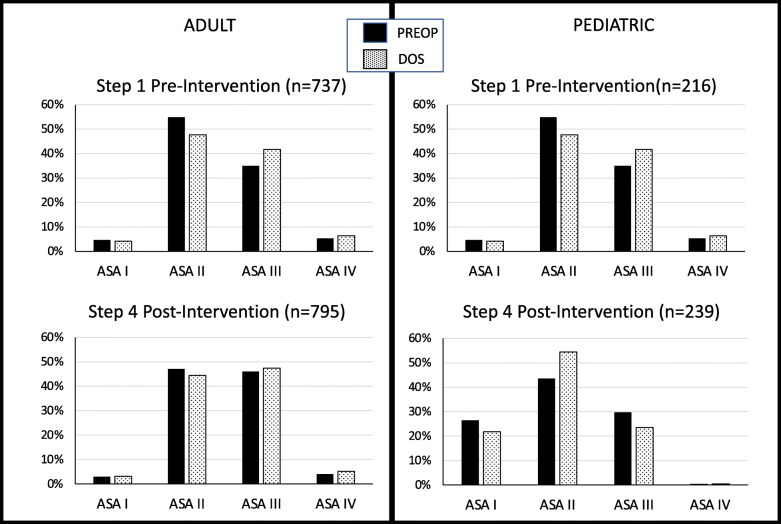
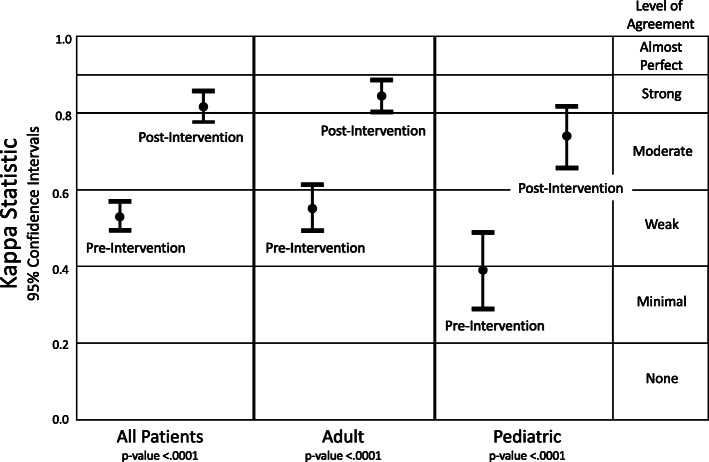
Methods: A multi-step, multi-year quality improvement project was performed. Step 1, pre-intervention, was a retrospective review to determine the percentage agreement of ASA PS assignment between APAC and DOS for adult and pediatric patients. Step 2 was a retrospective review of the step 1 cases where the ASA PS assignment differed to determine which medical conditions were valued differently and then develop institutional-specific examples for medical conditions not addressed by ASA-approved examples. Step 3 was to educate clinicians about the newly implemented examples and how they should be used as a guide. Step 4, post-intervention, was a retrospective review to determine if the examples improved agreement between APAC and DOS ASA PS assignments. Weighted Kappa coefficient was used to measure of interrater agreement excluding chance agreement.
Results: Having only ASA PS definitions available, APAC and DOS agreement was only 74% for adults (n = 737) and 63% for pediatric patients (n = 216). For adults, 20 medical co-morbidity categories and, for pediatric patients, 9 medical co-morbidity categories accounted for > 90% the differences in ASA PS. After development and implementation of institutional-specific examples with ASA-approved examples, the percentage agreement increased for adult patients (n = 795) to 91% and for pediatric patients (n = 239) to 84%. Weighted Kappa coefficients increased significantly for all patients (from 0.62 to 0.85, p < .0001), adult patients (from 0.62 to 0.86, p < .0001), and pediatric patients (from 0.48 to 0.78, p < .0001).
Conclusions: ASA-approved examples do not address all medical conditions that account for differences in the assignment of ASA PS between pre-anesthesia screening and day of anesthesia evaluation at our institution. The process of developing institutional-specific examples addressed the medical conditions that caused differences in assignment at one institution. The implementation of ASA PS examples improved consistency of assignment, and therefore communication of medical conditions of patients presenting for anesthesia care.
Keywords: Anesthesia; Perioperative care; Physical Status Classification; Preoperative care; Quality improvement.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Abouleish AE, Leib ML, Cohen NH. ASA provides examples to each ASA physical status class. ASA Monitor. 2015;79:38–39.
-
- Alpin S, Bains D, De Lima J. Use of the ASA physical status grading system in pediatric practice. Pediatr Anesth. 2007. 10.1111/j.1460-9592.2006.02094.x. - PubMed
-
- Altman DG. Practical statistics for medical research. London: Chapman and Hall/CRC Press; 1991. p. 404.
-
- American Society for Gastrointestinal Endoscopy. Sedation and anesthesia in GI endoscopy. Gastrointest Endosc. 2008. 10.1016/j.gie.2008.09.029. - PubMed
-
- Aronson S, Westover J, Guinn N, et al. A perioperative medicine model for population health: an integrated approach for an evolving clinical science. Anesth Analg. 2018. 10.1213/ANE.0000000000002606. - PubMed
LinkOut - more resources
Full Text Sources
