

Prevalence and prognostic value of elevated troponins in patients hospitalised for coronavirus disease 2019: a systematic review and meta-analysis
- PMID: 33292649
- PMCID: PMC7682759
- DOI: 10.1186/s40560-020-00508-6
Prevalence and prognostic value of elevated troponins in patients hospitalised for coronavirus disease 2019: a systematic review and meta-analysis
Abstract
Background: The clinical significance of cardiac troponin measurement in patients hospitalised for coronavirus disease 2019 (covid-19) is uncertain. We investigated the prevalence of elevated troponins in these patients and its prognostic value for predicting mortality.
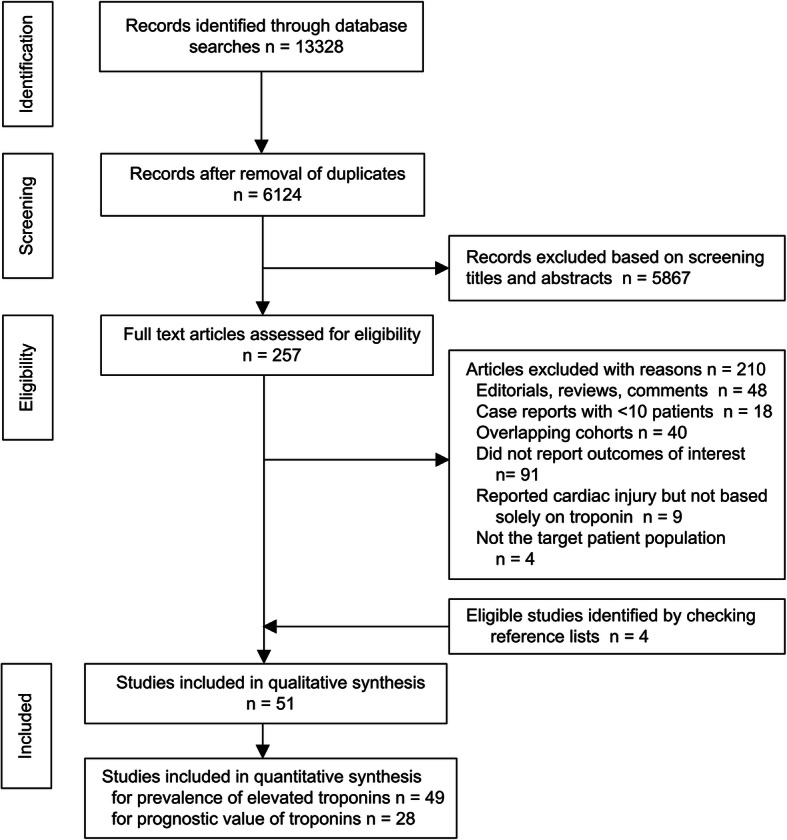
Methods: Studies were identified by searching electronic databases and preprint servers. We included studies of hospitalised covid-19 patients that reported the frequency of troponin elevations above the upper reference limit and/or the association between troponins and mortality. Meta-analyses were performed using random-effects models.
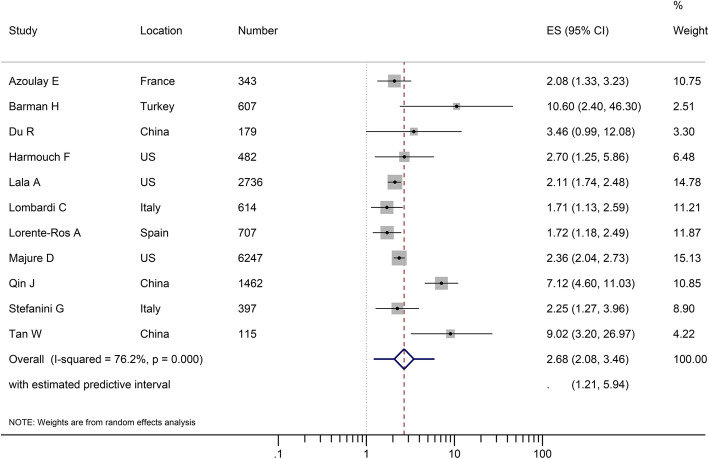
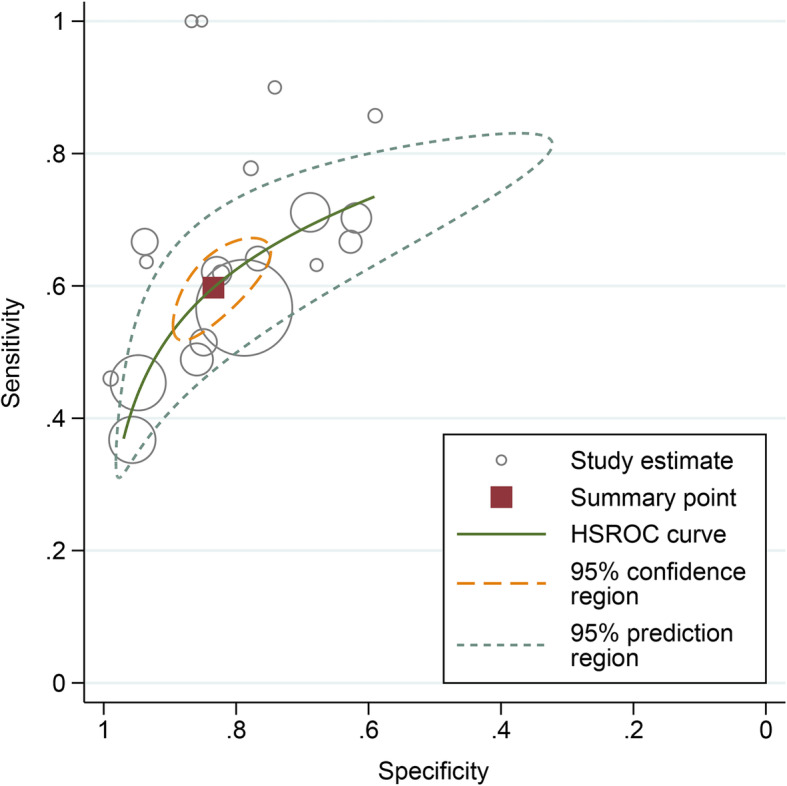
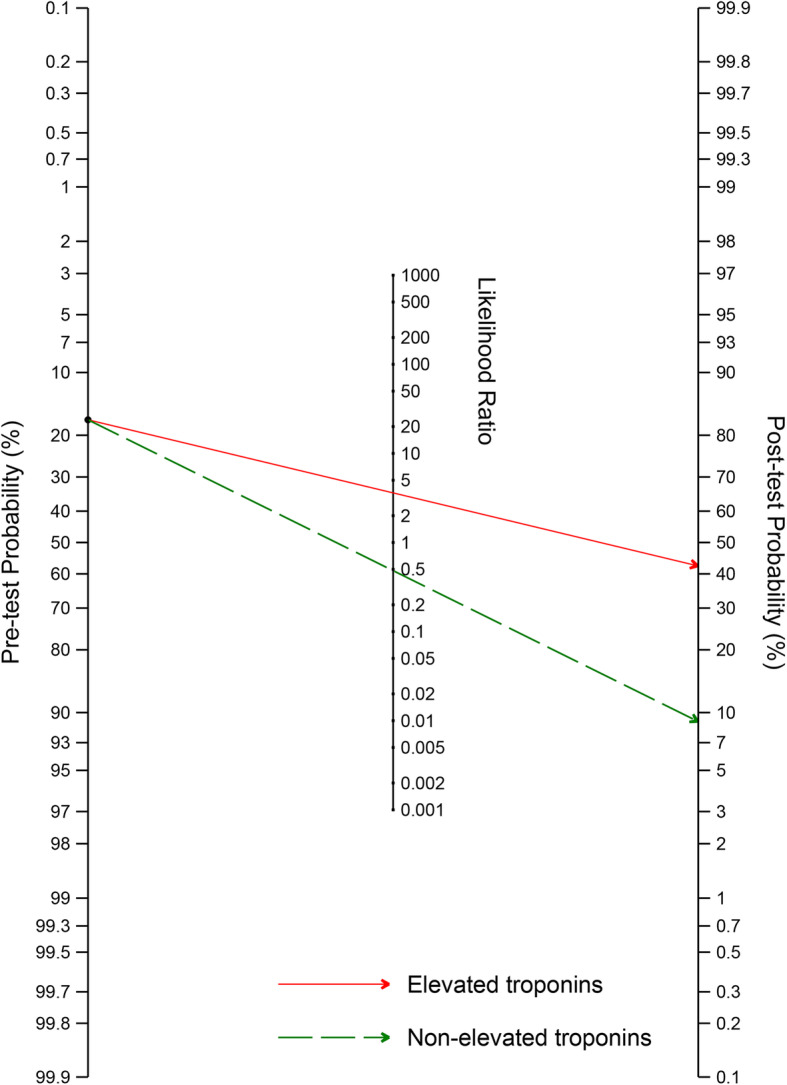
Results: Fifty-one studies were included. Elevated troponins were found in 20.8% (95% confidence interval [CI] 16.8-25.0 %) of patients who received troponin test on hospital admission. Elevated troponins on admission were associated with a higher risk of subsequent death (risk ratio 2.68, 95% CI 2.08-3.46) after adjusting for confounders in multivariable analysis. The pooled sensitivity of elevated admission troponins for predicting death was 0.60 (95% CI 0.54-0.65), and the specificity was 0.83 (0.77-0.88). The post-test probability of death was about 42% for patients with elevated admission troponins and was about 9% for those with non-elevated troponins on admission. There was significant heterogeneity in the analyses, and many included studies were at risk of bias due to the lack of systematic troponin measurement and inadequate follow-up.
Conclusion: Elevated troponins were relatively common in patients hospitalised for covid-19. Troponin measurement on admission might help in risk stratification, especially in identifying patients at high risk of death when troponin levels are elevated. High-quality prospective studies are needed to validate these findings.
Systematic review registration: PROSPERO CRD42020176747.
Keywords: Covid-19; Meta-analysis; Myocardial injury; Risk prediction; Troponin.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
