

Takotsubo syndrome induced by brachytherapy in a patient with endocervical adenocarcinoma
- PMID: 33292719
- PMCID: PMC7718687
- DOI: 10.1186/s40959-020-00082-8
Takotsubo syndrome induced by brachytherapy in a patient with endocervical adenocarcinoma
Abstract
Background: Takotsubo syndrome (TTS), also known as stress cardiomyopathy, apical ballooning syndrome and broken heart syndrome, is characterized by acute-onset chest pain, electrocardiographic (ECG) abnormalities and reversible left ventricular (LV) disfunction in the absence of a culprit obstructive lesion in the coronary arteries; therefore, myocardial infarction is the most important differential diagnosis. Usually induced by emotional/physical stress, its treatment consists in hemodynamic support until complete and spontaneous recovery occurs, which is generally achieved within a few days to weeks. Cervical malignancies are an important public health issue in low/middle-income countries and, in the setting of locally advanced disease, concurrent chemoradiation followed by brachytherapy is considered the standard treatment, harboring curative potential.
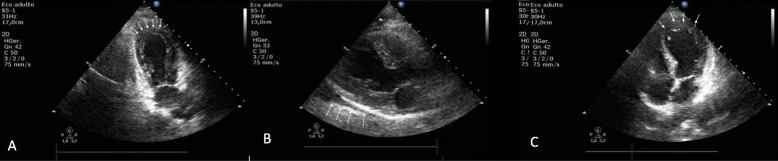
Case report: We report a case of a 38-year-old woman who underwent concurrent chemoradiotherapy and developed cardiopulmonary arrest in ventricular fibrillation during a brachytherapy session. Complementary tests disclosed altered ECG and cardiac biomarkers, no evidence of coronary artery obstruction, as well as LV disfunction consistent with TTS on echocardiogram and cardiac MRI. After few days of supportive therapy, complete recovery of heart function was observed.
Conclusions: Especially for cancer patients, who usually experience intense emotional/physical stress intrinsically associated with their diagnosis and aggressive treatments, considering TTS as a differential diagnosis is warranted. Intracavitary brachytherapy procedure may represent a trigger for TTS.
Keywords: Brachytherapy; Broken heart syndrome; Endocervical adenocarcinoma; Heart failure; Stress cardiomyopathy; Takotsubo.
Conflict of interest statement
The authors declare that they have no potential conflicts of interest related to this publication.
Figures


Similar articles
-
Cardiogenic shock due to reverse takotsubo syndrome triggered by multiple sclerosis brainstem lesions: a case report and mini review.Front Cardiovasc Med. 2023 May 3;10:1175644. doi: 10.3389/fcvm.2023.1175644. eCollection 2023. Front Cardiovasc Med. 2023. PMID: 37206102 Free PMC article.
-
Takotsubo Syndrome: Cardiotoxic Stress in the COVID Era.Mayo Clin Proc Innov Qual Outcomes. 2020 Dec;4(6):775-785. doi: 10.1016/j.mayocpiqo.2020.08.008. Epub 2020 Nov 30. Mayo Clin Proc Innov Qual Outcomes. 2020. PMID: 33283161 Free PMC article. Review.
-
Zumba-induced Takotsubo cardiomyopathy: a case report.J Med Case Rep. 2018 Jun 10;12(1):160. doi: 10.1186/s13256-018-1696-x. J Med Case Rep. 2018. PMID: 29885664 Free PMC article.
-
[Postpartum Takotsubo cardiomyopathy: case report].Rev Bras Ginecol Obstet. 2015 Nov;37(11):526-32. doi: 10.1590/SO100-720320150005391. Rev Bras Ginecol Obstet. 2015. PMID: 26561243 Portuguese.
-
[Takotsubo cardiomyopathy: report of the first case series in Serbia and review of the literature].Med Pregl. 2010 Jan-Feb;63(1-2):75-81. doi: 10.2298/mpns1002075p. Med Pregl. 2010. PMID: 20873314 Review. Serbian.
Cited by
-
Takotsubo Syndrome: Pathophysiology, Emerging Concepts, and Clinical Implications.Circulation. 2022 Mar 29;145(13):1002-1019. doi: 10.1161/CIRCULATIONAHA.121.055854. Epub 2022 Mar 28. Circulation. 2022. PMID: 35344411 Free PMC article. Review.
-
An Extensive Review on Imaging Diagnosis Methods in Takotsubo Syndrome.Rev Cardiovasc Med. 2023 Oct 20;24(10):300. doi: 10.31083/j.rcm2410300. eCollection 2023 Oct. Rev Cardiovasc Med. 2023. PMID: 39077560 Free PMC article. Review.
References
-
- Sato H. Tako-tsubo-like left ventricular dysfunction due to multivessel coronary spasm. In: Clinical Aspect of Myocardial Injury: From Ischemia to Heart Failure. Kagakuhyoronsha Publishing Co; 1990:56–64.
LinkOut - more resources
Full Text Sources