

Anatomical and functional outcomes of subthreshold micropulse laser versus intravitreal ranibizumab injection in treatment of diabetic macular edema
- PMID: 33292788
- PMCID: PMC7712611
- DOI: 10.1186/s40942-020-00265-6
Anatomical and functional outcomes of subthreshold micropulse laser versus intravitreal ranibizumab injection in treatment of diabetic macular edema
Abstract
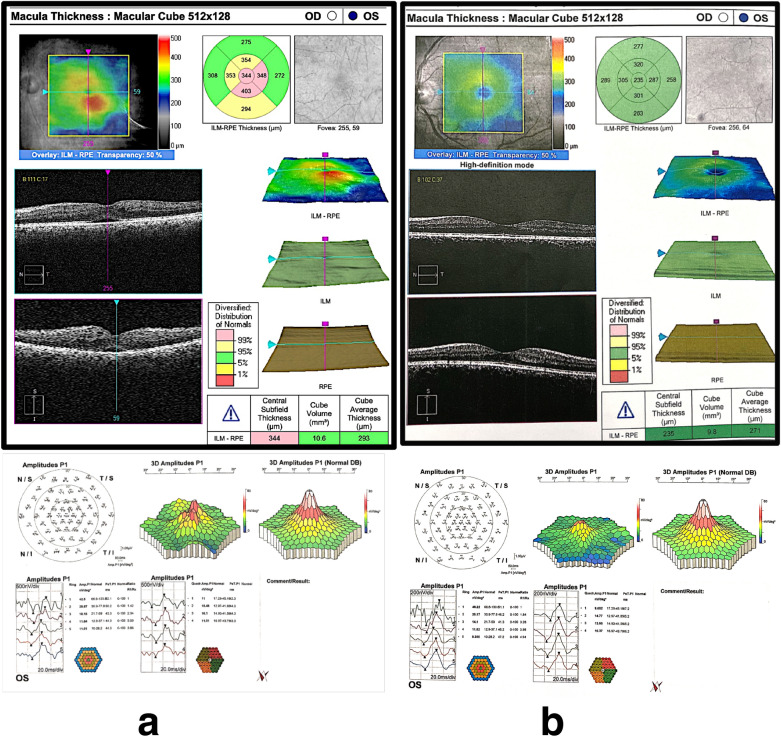
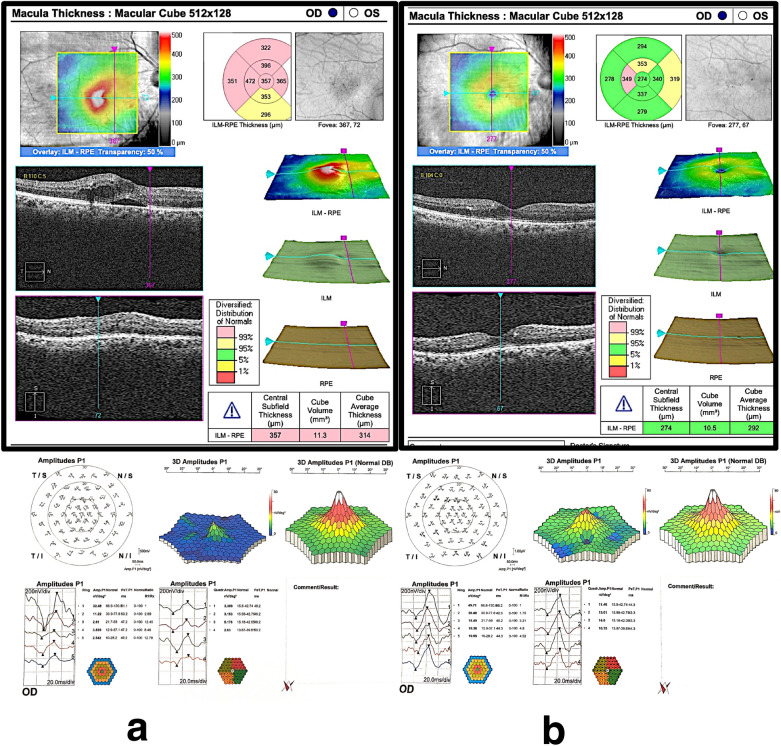
Background: To compare the therapeutic effects of subthreshold micropulse laser (SML) versus intravitreal injection of ranibizumab in treatment of diabetic macular edema (DME) both anatomically using optical coherence tomography (OCT) and functionally using best corrected visual acuity (BCVA) and multifocal electroretinogram (mfERG).
Methods: his study was an interventional prospective randomized comparative study. The study included 120 eyes classified into 3 groups: Group 1 included 40 eyes of 28 patients treated by SML laser, group 2 included 40 eyes of 32 patients treated by intravitreal injection of ranibizumab, and group 3 (control group for mfERG) included 40 eyes of 20 patients with diabetes mellitus (DM) of more than 10 year duration with no signs of diabetic retinopathy (DR). BCVA measurements, OCT and mfERG were done for the cases before and after interference and were followed up for 6 months RESULTS: By the end of the follow up period, BCVA significantly improved by 31% in group 1 vs 93% in group 2 with a statistically highly significant difference between the two groups (p value < 0.001). There was also a significant decrease in central subfield thickness in both groups with more reduction in group 2 compared with group 1 (p value < 0.001). There was a significant improvement in P1 amplitude of mf-ERG in group 2 (p value < 0.002) with no significant improvement in group 1. There was a significant decrease in P1 implicit time in group 2 (p value < 0.001) while there was no significant decrease in group1.
Conclusions: Intravitreal injection of ranibizumab is a superior treatment modality for DME compared with SML regarding both anatomical and functional outcomes.
Trial registration: This study has been approved by the local ethical committee of faculty of medicine of Minia University and retrospectively registered at the clinical trial gov. with Identifier: NCT04332133.
Keywords: Diabetic macular edema; Multifocal electroretinogram; Ranibizumab; Subthreshold micropulse laser.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Multifocal electroretinography changes at the 1-year follow-up in a cohort of diabetic macular edema patients treated with ranibizumab.Doc Ophthalmol. 2017 Oct;135(2):85-96. doi: 10.1007/s10633-017-9601-2. Epub 2017 Aug 4. Doc Ophthalmol. 2017. PMID: 28779336 Free PMC article.
-
Comparison of ranibizumab and subthreshold micropulse laser in treatment of macular edema secondary to branch retinal vein occlusion.Eur J Ophthalmol. 2018 Nov;28(6):690-696. doi: 10.1177/1120672117750056. Epub 2018 Apr 26. Eur J Ophthalmol. 2018. PMID: 29696993
-
Short pulse grid and subthreshold micropulse laser (the sandwich grid) plus intravitreal ranibizumab for the treatment of diabetic macular edema.Int J Retina Vitreous. 2024 Sep 30;10(1):69. doi: 10.1186/s40942-024-00585-x. Int J Retina Vitreous. 2024. PMID: 39350273 Free PMC article.
-
Practical Lessons from Protocol I for the Management of Diabetic Macular Edema.Dev Ophthalmol. 2017;60:91-108. doi: 10.1159/000459692. Epub 2017 Apr 20. Dev Ophthalmol. 2017. PMID: 28427069 Review.
-
Intravitreal Ranibizumab in Diabetic Macular Edema: Long-Term Outcomes.Dev Ophthalmol. 2017;60:63-70. doi: 10.1159/000460496. Epub 2017 Apr 20. Dev Ophthalmol. 2017. PMID: 28427066 Review.
Cited by
-
Subthreshold Micropulse Laser for Diabetic Macular Edema: A Review.J Clin Med. 2022 Dec 29;12(1):274. doi: 10.3390/jcm12010274. J Clin Med. 2022. PMID: 36615074 Free PMC article. Review.
-
Adjunct Nondamaging Focal Laser Reduces Intravitreal Injection Burden in Diabetic Macular Edema.Photonics. 2023 Oct;10(10):1165. doi: 10.3390/photonics10101165. Epub 2023 Oct 18. Photonics. 2023. PMID: 39006749 Free PMC article.
-
Subthreshold micropulse diode laser treatment in diabetic macular edema: biological impact, therapeutic effects, and safety.Int Ophthalmol. 2024 Feb 3;44(1):3. doi: 10.1007/s10792-024-02973-6. Int Ophthalmol. 2024. PMID: 38315299 Review.
References
-
- Fortune B, Schneck ME, Adams AJ. Multifocal electroretinogram delays reveal local retinal dysfunction in early diabetic retinopathy. Invest Ophthalmol Vis Sci. 1999;40:2638–51. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
