

Input from multiple stakeholder levels prioritizes targets for improving implementation of an exercise intervention for rural women cancer survivors
- PMID: 33292813
- PMCID: PMC7640400
- DOI: 10.1186/s43058-020-00061-1
Input from multiple stakeholder levels prioritizes targets for improving implementation of an exercise intervention for rural women cancer survivors
Abstract
Background: Although evidence-based interventions for increasing exercise among cancer survivors (CSs) exist, little is known about factors (e.g., implementation facilitators) that increase effectiveness and reach of such interventions, especially in rural settings. Such factors can be used to design implementation strategies. Hence, our study purpose was to (1) obtain multilevel perspectives on improving participation in and implementation of a multicomponent exercise behavior change intervention for rural women CSs and (2) identify factors important for understanding the context using the Consolidated Framework for Implementation Research (CFIR) for comparison across three levels (CSs, potential interventionists, community/organizational stakeholders).
Methods: We conducted three nominal group technique meetings with rural women CSs, three with community/organizational stakeholders, and one with potential interventionists. During each meeting, participants were asked to respond silently to one question asking what would make a multicomponent exercise intervention doable from intervention participation (CSs) or implementation (potential interventionists, stakeholders) perspectives. Responses were shared, discussed to clarify meaning, and prioritized by group vote. Data was deductively coded using CFIR.
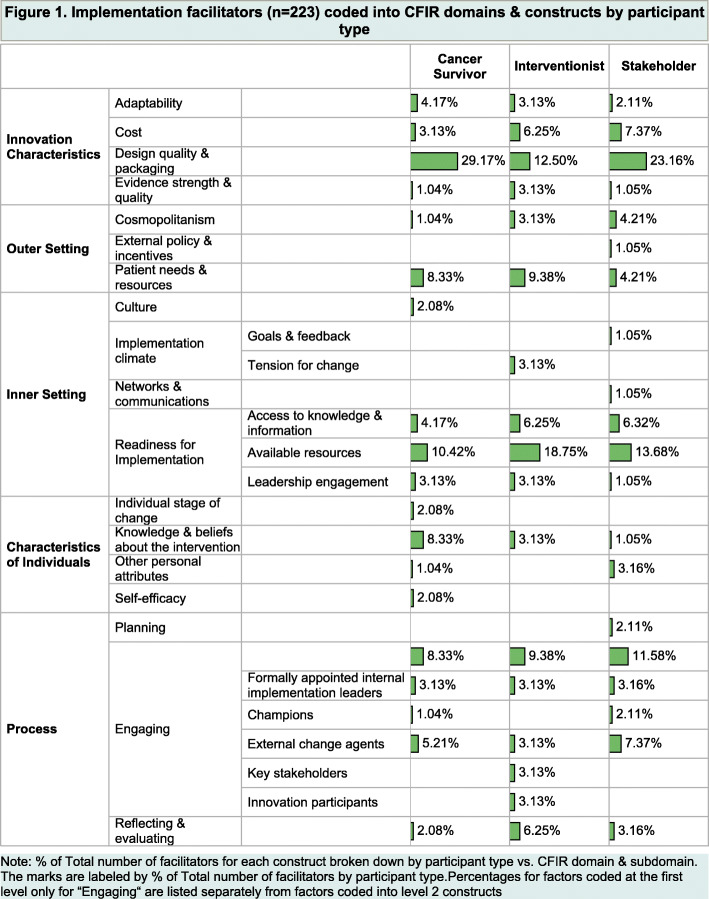
Results: Mean age of CSs (n = 19) was 61.8 ± 11.1 years, community stakeholders (n = 16) was 45.9 ± 8.1 years, and potential interventionists (n = 7) was 41.7 ± 15.2 years. There was considerable consensus among CSs, potential interventionists, and stakeholders in terms of CFIR domains and constructs, e.g., "Design quality and packaging" (Innovation Characteristics), "Patients needs and resources" (Outer Setting), "Available resources" (Inner Setting), and "Engaging" (Process). However, participant-specific CFIR domains and constructs were also observed, e.g., CSs endorsed "Knowledge and beliefs about the intervention," "Individual stage of change," and "Self-efficacy" (Characteristics of Individuals); potential interventionists valued "Tension for change" (Inner Setting) and "Innovation participants" and "Key stakeholder" (Process); stakeholders emphasized "Goals and feedback" and "Network and communication" (Inner Setting), and "Planning" (Process). How the three participant levels conceptualized the CFIR constructs demonstrated both similarities and differences.
Conclusions: Multilevel input yielded diversity in type, relative priority, and conceptualization of implementation facilitators suggesting foci for future implementation strategy development and testing. Findings also reinforced the importance of multilevel implementation strategies for increasing exercise in an underserved, at-risk population.
Keywords: Health promotion; Implementation; Nominal group technique; Oncology; Physical activity; Qualitative; Survivorship.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Bradshaw PT, Ibrahim JG, Khankari N, Cleveland RJ, Abrahamson PE, Stevens J, Satia JA, Teitelbaum SL, Neugut AI, Gammon MD. Post-diagnosis physical activity and survival after breast cancer diagnosis: the Long Island Breast Cancer Study. Breast Cancer Res Treat. 2014;145(3):735–742. doi: 10.1007/s10549-014-2966-y. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
