

Low dose ionizing radiation effects on the immune system
- PMID: 33293042
- PMCID: PMC8784945
- DOI: 10.1016/j.envint.2020.106212
Low dose ionizing radiation effects on the immune system
Abstract
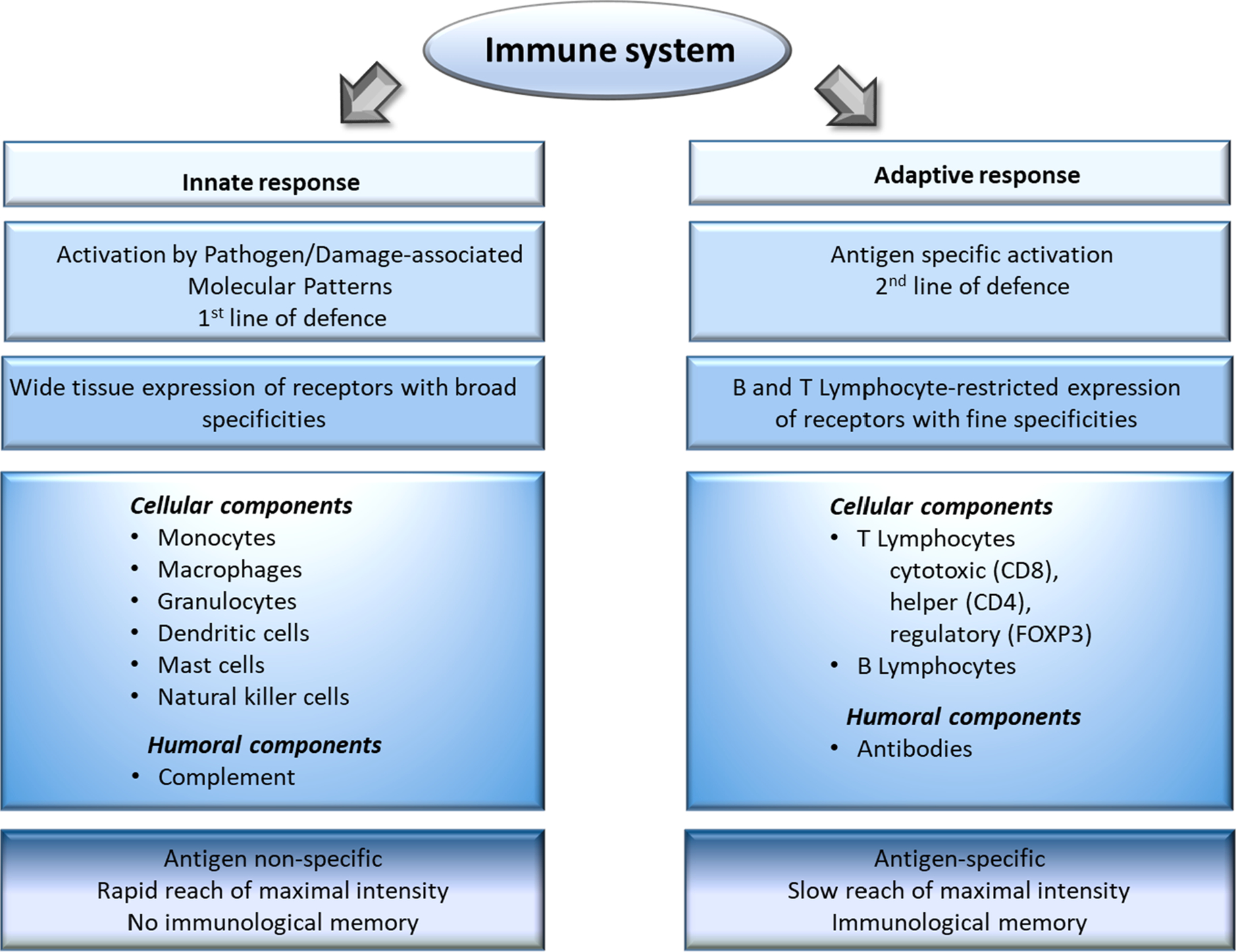
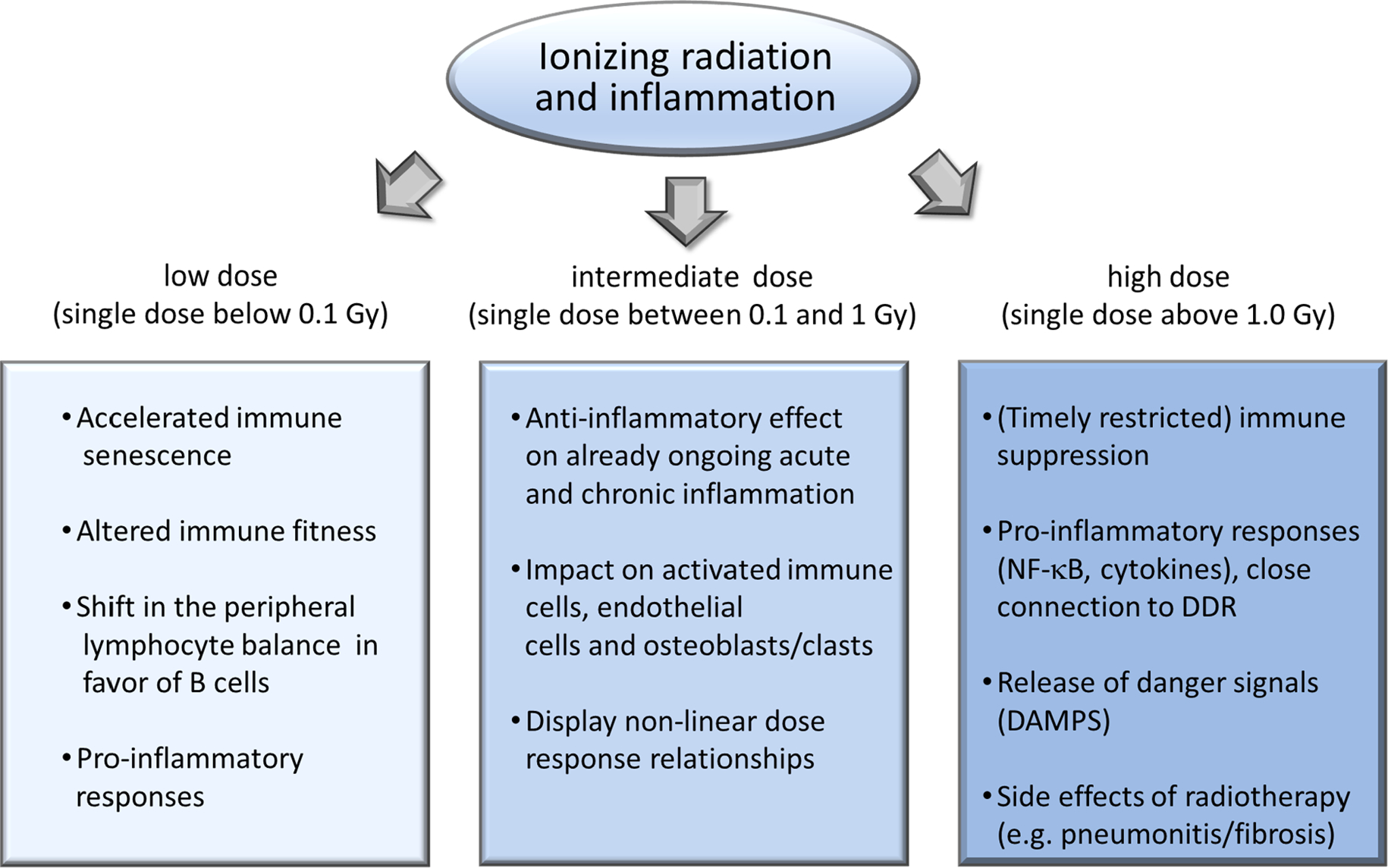
Ionizing radiation interacts with the immune system in many ways with a multiplicity that mirrors the complexity of the immune system itself: namely the need to maintain a delicate balance between different compartments, cells and soluble factors that work collectively to protect, maintain, and restore tissue function in the face of severe challenges including radiation damage. The cytotoxic effects of high dose radiation are less relevant after low dose exposure, where subtle quantitative and functional effects predominate that may go unnoticed until late after exposure or after a second challenge reveals or exacerbates the effects. For example, low doses may permanently alter immune fitness and therefore accelerate immune senescence and pave the way for a wide spectrum of possible pathophysiological events, including early-onset of age-related degenerative disorders and cancer. By contrast, the so called low dose radiation therapy displays beneficial, anti-inflammatory and pain relieving properties in chronic inflammatory and degenerative diseases. In this review, epidemiological, clinical and experimental data regarding the effects of low-dose radiation on the homeostasis and functional integrity of immune cells will be discussed, as will be the role of immune-mediated mechanisms in the systemic manifestation of localized exposures such as inflammatory reactions. The central conclusion is that ionizing radiation fundamentally and durably reshapes the immune system. Further, the importance of discovery of immunological pathways for modifying radiation resilience amongst other research directions in this field is implied.
Keywords: DNA damage response; Epidemiological data; Immune system; Inflammation; Low-dose ionizing radiation.
Copyright © 2020 The Authors. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
-
- Agate L, Mariotti S, Elisei R, Mossa P, Pacini F, Molinaro E, Grasso L, Masserini L, Mokhort T, Vorontsova T, Arynchyn A, Tronko MD, Tsyb A, Feldt-Rasmussen U, Juul A, Pinchera A, 2008. Thyroid autoantibodies and thyroid function in subjects exposed to Chernobyl fallout during childhood: evidence for a transient radiation-induced elevation of serum thyroid antibodies without an increase in thyroid autoimmune disease. J. Clin. Endocrinol. Metab. 93, 2729–2736. 10.1210/jc.2008-0060. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
