

Anti-inflammatory therapy for COVID-19 infection: the case for colchicine
- PMID: 33293273
- PMCID: PMC8491433
- DOI: 10.1136/annrheumdis-2020-219174
Anti-inflammatory therapy for COVID-19 infection: the case for colchicine
Abstract
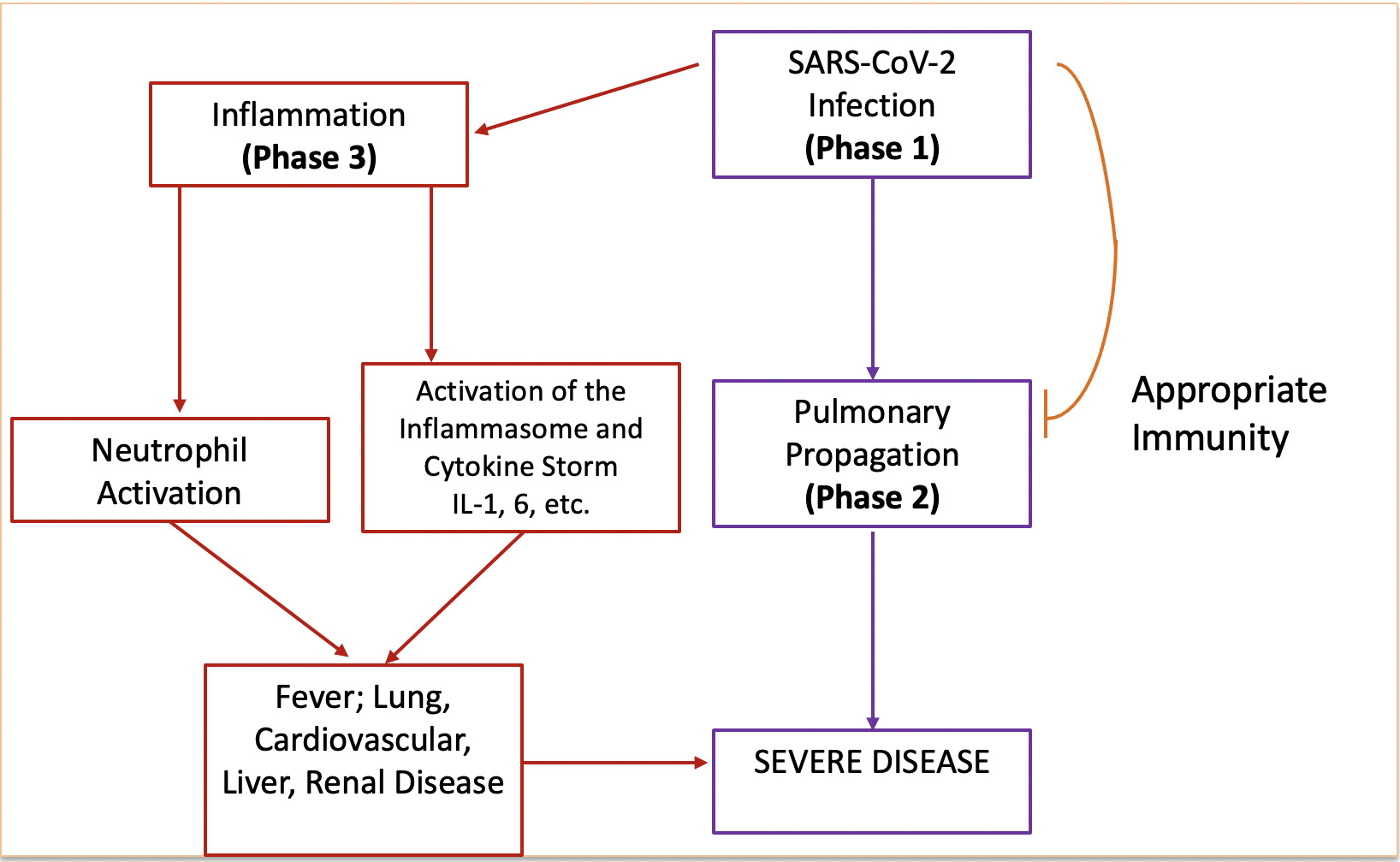
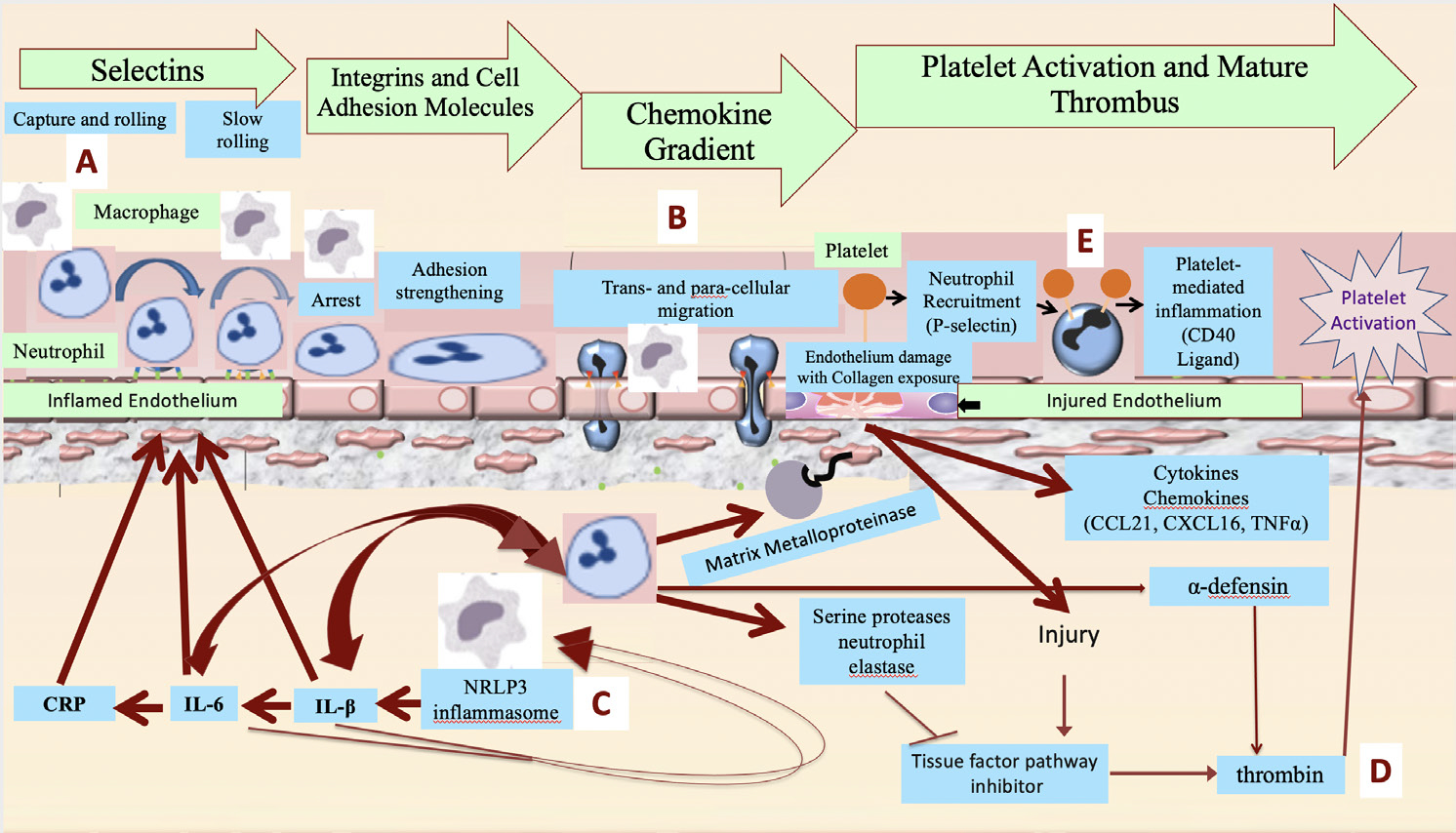
The search for effective COVID-19 management strategies continues to evolve. Current understanding of SARS-CoV-2 mechanisms suggests a central role for exaggerated activation of the innate immune system as an important contributor to COVID-19 adverse outcomes. The actions of colchicine, one of the oldest anti-inflammatory therapeutics, target multiple mechanisms associated with COVID-19 excessive inflammation. While many COVID-19 trials have sought to manipulate SARS-CoV-2 or dampen the inflammatory response once patients are hospitalised, few examine therapeutics to prevent the need for hospitalisation. Colchicine is easily administered, generally well tolerated and inexpensive, and holds particular promise to reduce the risk of hospitalisation and mortality due to COVID-19 in the outpatient setting. Successful outpatient treatment of COVID-19 could greatly reduce morbidity, mortality and the demand for rare or expensive care resources (front-line healthcare workers, hospital beds, ventilators, biological therapies), to the benefit of both resource-replete and resource-poor regions.
Keywords: chemokines; cytokines; immune system diseases; inflammation; therapeutics.
© Author(s) (or their employer(s)) 2021. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: For the purposes of full disclosure, we note that BS receives support from the NIH/NHLBI (1R01HL146206, 3R01HL146206-02S1) and VA ORD (iK2CX001074) for her work on colchicine in cardiovascular disease and COVID-19. J-CT reports grants and personal fees from Amarin, grants and personal fees from AstraZeneca, grants, personal fees and other from DalCor, grants from Esperion, grants from Ionis, grants and personal fees from Pfizer, grants and personal fees from Sanofi, grants and personal fees from Servier, personal fees from HLS Therapeutics, outside the submitted work; In addition, J-CT has a patent on pharmacogenomics-guided CETP inhibition issued, and a patent on the use of colchicine after myocardial infarction pending. MHP holds investigator-initiated grants from Horizon Therapeutics (to study urate deposition in the spines of gout patients) and Hikma Pharmaceuticals (to study the possible benefit of colchicine in knee osteoarthritis) and has served as a consultant for Horizon and Sobi. MHP also receives salary support from a CTSA award (1UL1TR001445) to New York University from the National Centre for the Advancement of Translational Science, National Institutes of Health. TLWM is supported by an NYU‐HHC Clinical and Translational Science Institute KL2 grant and a Doris Duke Fund to Retain Clinical Scientists award. TLWM has served on an advisory board for Novartis and as a consultant to Regeneron, unrelated to this work
Figures
Comment in
-
Correspondence on 'Anti-inflammatory therapy for COVID-19 infection: the case for colchicine'.Ann Rheum Dis. 2023 Apr;82(4):e81. doi: 10.1136/annrheumdis-2021-219872. Epub 2021 Jan 28. Ann Rheum Dis. 2023. PMID: 33509794 No abstract available.
-
Response to: 'Correspondence on 'Anti-inflammatory therapy for COVID-19 infection: the case for colchicine'' by Perricone et al.Ann Rheum Dis. 2023 Apr;82(4):e82. doi: 10.1136/annrheumdis-2021-219898. Epub 2021 Jan 28. Ann Rheum Dis. 2023. PMID: 33509798 No abstract available.
References
-
- Schroder K, Tschopp J. The inflammasomes. Cell 2010;140:821–32. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
